Download
1 / 35
400 likes | 482 Views
Exploring the initiation and mechanisms behind bacterial disease development, host-pathogen interaction, and Koch's postulates in linking bacteria to diseases. Learn about pathogenicity, virulence traits, and the role of the host's immune system in determining disease outcomes.

E N D
PATHOGENESISOFBACTERIAL INFECTION PATHOGENICITYVIRULENCE
Thepathogenesisofbacterialinfectionincludestheinitiationoftheinfectiousprocessandthemechanismsleading to thedevelopmentofsignsandsymptomsofbacterialdisease. • Theoutcomeoftheinteractionbetweenbacteriaand host isdetermined by characteristicsthatfavour establishment ofthebacteriawithinthe host andtheirability to damagethe host as they are opposed by host defense mechanisms.
Amongthecharactericsofbacteria are adherence to host cells, invasiveness, toxigenity, andability to evadethe host´s immunesystem. • Ifthebacteriaorimmunologicalreactionsinjurethe host sufficiently, diseasebecomesapparent.
Pathogenesis of bacterial infection • Humans and animals have abundant normal microflora. • Most bacteria do not produce disease but achieve a balance with the host that ensures the survival, growth, and propagation of both the bacteria and the host. • Sometimes bacteria that are clearly pathogens (e.g. Salmonella typhi) are present, but infection remains latent or subclinical and the host is a "carrier" of the bacteria.
It can be difficult to show that a specific bacterial species is the cause of a particular disease. In 1884, Robert Koch proposed a series of postulates in his treatise on Mycobacterium tuberculosis and tuberculosis. These postulates have been applied more broadly to link many specific bacterial species with particular diseases.
Koch´s postulates are summarized as follows: • The microorganism should be found in all cases of the disease in question, and its distribution in the body should be in accordancce with the lesions observed. • The microorganism should be grown in pure culture in vitro (or outsite the body of the host) for several generations. • When such a pure culture is inoculated into susceptible animal species, the typical disease must result. • The microorganism must again be isolated from the lesions of such experimentally produced disease.
Koch´s postulatesremain a mainstayofmicrobiology.However, sincethelate 19th century, many microorganismsthat do not meetthecriteriaofthepostulateshavebeenshown to cause disease. Forexample, Treponema pallidum (syphilis) andMycobaceriumleprae (leprosy) cannotbegrown in vitro, butthere are animalmodelsofinfectionwith these agents.
In another example, Neisseria gonorrhoeae (gonorrhea), there is no animal model of infection even though the bacteria can readily be cultivated in vitro.The host´s immune responses should be considered when an organism is being investigated as the possible cause of a disease. Thus, development of a rise in specific antibody during recovery from disease is an important adjunct to Koch´s postulates.
Modern-day microbial genetics has opened new frontiers to study pathogenic bacteria and differentiate them from non-pathogens. The ability to study genes associated with virulence has led to a proposed of Koch´s postulates: • The phenotype, or property, under investigation should be associated with pathogenic members of a genus or pathogenic strains of a species. • Specific inactivation of the gene(s) associated with the suspected virulence trait should lead to a measurable loss in pathogenicity or virulence. • Reversion or allelic replacement of the mutated gene should lead to restoration of pathogenicity.
Analysisofinfectionanddiseasethroughtheapplicationofprinciples such as Koch´s postulatesleads to classificationofbacteria as pathogenicor non-pathogenic. • Somebacterial species are alwaysconsidered to bepathogens, andtheir presence isabnormal. • ExamplesincludeMycobacteriumtuberculosis (tuberculosis) andYersiniapestis (plague). • Other species are commonly part ofthenormal flora ofhumans (andanimals) butcanalsofrequently cause disease. Forexample, Escherichiacoliis part ofthegastrointestinal flora ofnormalhumans, butitisalso a comon cause ofurinarytractinfection, traveller´s diarrhea, andotherdiseases.
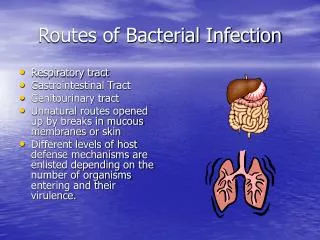
The infectious process • Infection indicates multiplication of microorganisms. • Prior to multiplication, bacteria (in case of bacterial infection) must enter and establish themselves within the host. • The most frequent portals of entry are the respiratory (mouth and nose), gastrointestinal, and urogenital tracts. Abnormal areas of mucous membranes and skin (e.g. cuts, burns) are also frequent sites of entry.
The infectious process • Once in the body, bacteriamustattachoradhere to host cells, usuallyepithelialcells. • Afterthebacteriahaveestablished a primarysiteofinfection, they multiply andspread. • Infectioncanspreaddirectlythroughtissuesor via thelymphaticsystem to bloodstream. Bloodstreaminfection (bacteremia) canbetransientorpersistent. Bacteremiaallowsbacteria to spreadwidely in the body andpermitsthem to reachtissuesparticularlysuitablefortheirmultiplication.
The infectious process • As anexampleoftheinfectiousprocess, Streptococcuspneumoniaecanbeculturedfromthenasopharynxof 5-40% ofhealthypeople. • Occasionally, Streptococcuspneumoniaestrainsfromthenasopharynx are aspiratedintothelungs. Infectiondevelops in theterminalairspaceofthelungs in personswho do not haveprotectiveantibodiesagainstthat type ofStreptococcuspneumoniae. MultiplicationofStreptococcuspneumoniaestrainsand resultant inflammationlead to pneumonia. Thestrainsthen enter thelymphaticsofthelungandmove to thebloodstream. Between 10% and 20% ofpersonswithStreptococcuspneumoniaepneumoniahavebacteremiaatthetimethediagnosisofpneumoniaismade. Oncebacteremiaoccurs, Streptococcuspneumoniaestrainscanspread to theirpreferredsecondarysitesofinfection (e.g. cerebrospinal fluid, heartvalves, joint spaces). The major resultingcomplicationsofStreptococcuspneumoniaepneumoniainclude meningitis, endocarditisandseptic arthritis.
Basic termsfrequentlyused in describingaspectsofpathogenesis: • Infection: • Multiplicationofaninfectious agent withinthe body. • Multiplicationofthebacteriathat are part ofnormal flora ofgastrointestinaltract, skin, etc, isgenerally not consideredaninfection. • On theotherhand, multiplicationofpathogenicbacteria (e.g. Salmonella species), evenifthe person isasymptomatic, isdeemedaninfection.
Basic termsfrequentlyused in describingaspectsofpathogenesis: • Pathogenicity: • Theabilityofaninfectious agent to cause disease. • Virulence: • Thequantitativeabilityofan agent to cause disease. • Virulentagents cause diseasewhenintroducedintothe host in smallnumbers. • Virulence involvesinvasivenessandtoxigenicity.
Basic termsfrequentlyused in describingaspectsofpathogenesis: • Toxigenicity: • Theabilityof a microorganism to produce a toxin thatcontributes to thedevelopmentofdisease. • Invasion: • Theprocesswherebybacteria, parasites, fungiandviruses enter the host cellsortissuesandspread in the body.
Basic termsfrequentlyused in describingaspectsofpathogenesis: • Pathogen: • A microorganismcapableofcausingdisease. • Non-pathogen: • A microorganismthatdoes not cause disease. Itmaybe part ofthenormal flora. • Opportunisticpathogen: • An agent capableofcausingdiseaseonlywhenthe host´s resistanceisimpaired (e.g. thepatientisimmunocompromised). • An agent capableofcausingdiseaseonlywhenspreadfromthesitewithnormalbacterialmicroflora to thesteriletissueor organ.
Bacterial virulence factors • Many factorsdeterminethe virulence ofbacteria, ortheirability to cause infectionanddisease.
Toxins • Toxinsproduced by bacteria are generallyclassifiedintotwogroups: • exotoxins • endotoxins
Endotoxinsof gram-negative bacteria • Theendotoxinsof gram-negative bacteria are derivedfrombacterial cell wallsand are oftenliberatedwhenthebacteria lyse. • Thesubstances are heat-stableandcanbeextracted (e.g. withphenol-water).
Pathophysiologicaleffectsofendotoxins are similarregardlessoftheirbacterialorigin: • fever • leukopenia • hypotension • impaired organ perfusionandacidosis • activationof C3 andcomplementcascade • disseminatedintravascularcoagulation (DIC) • death
Exotoxins • Many gram-positive and gram-negative bacteriaproduceexotoxinsofconsiderablemedicalimportance. • Someof these toxinshave had major role in worldhistory (e.g. toxin ofClostridium tetani).
Diphtheria toxin(toxin ofCorynebacteriumdiphtheriae) • Corynebacteriumdiphtheriaestrainsthatcarry a temperatebacteriophagewiththestructural gene forthe toxin are toxigenicandproducediphtheria toxin. • Thisnative toxin isenzymaticallydegradedintotwofragments: A and B, linkedtogether by a disulfide bound. Bothfragments are necessaryfor toxin activity.
Tetanospasmin (toxin of Clostridium tetani) • Clostridium tetaniisananaerobic gram-positive rod thatiswidespread in theenvironment. • Clostridium tetanicontaminateswounds, andthesporesgerminate in theanaerobicenvironmentofthedevitalizedtissue. ThevegetativeformsofClostridium tetaniproduce toxin tetanospasmin. Thereleased toxin has twopeptideslinked by disulfide bounds. Toxin reachesthecentralnervoussystem by retrograde transport alongaxonsandthroughthesystemiccirculation. The toxin acts by blockingreleaseofan inhibitory mediator in motor neuron synapses. Theresultisinitiallylocalizedthengeneralized, musclespasms. Extremelysmallamountof toxin canbelethalforhumans.
Botulotoxin (toxin of Clostridium botulinum) • Clostridium botulinumisfound in soilorwaterandmaygrow in foodsiftheenvironmentisappropriatelyanaerobic. • Anexceedinglypotent toxin (the most potent toxin known) isproduced by Clostridium botulinumstrains. Itisheat-labileandisdestroyed by sufficientheating. There are eightdisctinctserologicaltypesof toxin. Types A, B and E are most commonlyassociatedwihhumandisease. Toxin isabsorbedfromthe gut andcarried to motor nerves, whereitblocksthereleaseof acetylcholine atsynapsesandneuromuscularjunctions. Musclecontractiondoes not occur, andparalysisresults.
ToxinsofClostridium perfringens • SporesofClostridium perfringens are introducedintothewounds by contaminationwithsoilorfaeces. In the presence ofnecrotictissue (ananaerobicenvironment), sporesgerminateandvegetativecellsproduceseveraldifferenttoxins. • Many of these are necrotizingandhemolyticandfavourthespreadofgangrene: • alpha toxin is a lecithinasethatdamages cell membranes • theta toxin also has a necrotizingaffect • andother
Streptococcalerythrogenic toxin • Somestrainsofhemolyticlysogenicstreptococciproduce a toxin thatresults in a punctatemaculopapularerythematousrash, as in scarletfewer. • Productionoferythrogenic toxin isunderthegeneticcontroloftemperatebacteriophage. Ifthephageislost, thestreptococicannotproduce toxin.
Toxicshock syndrom toxin - 1 (TSST-1) • SomeStaphylococcus aureusstrainsgrowing on mucousmembranes (e.g. on the vagina in associationwithmenstruation), or in wounds, elaborate TSST-1. • Althoughthe toxin has beenassociatedwithtoxicshock syndrome, themechanismofaction in unknown. • Theillnessischaracterized by shock, highfewer, and a diffuseredrashthatlaterdesquamates, multiple otherorganssystems are involved as well.
Exotoxinsassociatedwithdiarrhealdiseases • Vibrio cholerae toxin • Staphylococcus aureus enterotoxin • Otherenterotoxins - enterotoxins are alsoproduced by somestrainsof: • Yersiniaenterocolitica • Vibrio parahaemolyticus • Aeromonas species
Enzymes • Many species ofbacteriaproduceenzymesthat are not intrinsicallytoxicbut play important role in theinfectiousprocess. • Collagenase: • degradescollagen, the major protein offibrousconnectivetissue, andpromotesspreadofinfection in tissue. • Coagulase: • Staphylococcus aureusproducecoagulase, whichworks in conjuctionwithserumfactors to coagulate plasma. Coagulasecontributes to theformationof fibrin wallsaroundstaphylococcallesions, whichhelpsthempersist in tissues.
Enzymes • Hyaluronidases: • enzymesthathydrolyzehyaluronicacid, a constituentoftheground substance ofconnectivetissue. They are produced bymany bacteria (e.g. staphylococci, streptococciandanaerobes) andaid in theirspreadthroughtissues. • Streptokinase: • many hemolyticstreptococciproducestreptokinase (fibrinolysin), substance thatactivates a proteolytic enzyme of plasma. This enzyme, alsocalledfibrinolysin, isthenable to dissolvecoagulated plasma andprobably aids in thespreadofstreptococcithroughtissues. Streptokinaseisused intreatmentofacutemyocardialinfarction to dissolve fibrin clots.
Enzymes • Hemolysinsandleukocidins: • Many bacteriaproducesubstancesthat are cytolysins - theydissolveredbloodcells (hemolysins) orkilltissuecellsorleukocytes (leukocidins). • Streptolysin O, forexample, isproduced by group A streptococciandisletalformiceandhemolyticforredbloodcellsfrom many animals.
Antiphagocyticfactors • Many bacterialpathogens are rapidlykilledoncethey are ingested by polymorphonuclearcellsormacrophages. • Somepathogensevadephagocytosisor leukocyte microbidicalmechanisms by adsorbingnormal host componets to theirsurfaces. • Forexample, Staphylococcus aureus has surface protein A, whichbinds to theFcportionofIgG. Otherpathogenshavesurfacefactorsthatimpedephagocytosise.g. Streptococcuspneumoniaeand many otherbacteriahavepolysaccharidecapsules.
Adherence factors • Oncebacteria enter the body ofthe host, theymustadhere to cellsof a tissuesurface. Ifthey do not adhere, theywouldbesweptaway by mucusandotherfluidsthatbathethetissuesurface. • Adherence (whichisonlyone step in theinfectiousprocess) isfollowed by developmentofmicrocoloniesandsubsequentcomplexsteps in thepathogenesisofinfection.
Adherence factors • Theinteractionsbetweenbacteriaandtissue cell surfaces in theadhesionprocess are complex. • Severalfactors play important role: • surfacehydrophobicity • bindingmolecules on bacteriaand host cell receptor interaction • andother