Download
1 / 14
220 likes | 799 Views
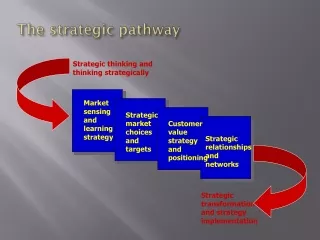
The Grampian Stroke Pathway. Acute Stroke Unit. Patient pathway. Patient has stroke/TIA. Red is BAD. NHS 24 . GP. A&E. Clinic. Stroke bleep notified. D.o.M.E. AMAU. Acute Stroke Unit. Decant/ things get missed. Vascular. M.S.T. Community hospitals. Home. Ward 12 WE. Ward 6 WE.

E N D
The Grampian Stroke Pathway Acute Stroke Unit
Patient pathway Patient has stroke/TIA Red is BAD NHS 24 GP A&E Clinic Stroke bleep notified D.o.M.E. AMAU Acute Stroke Unit Decant/ things get missed Vascular M.S.T. Community hospitals Home Ward 12 WE Ward 6 WE Care home/ interim care GP and primary care team CHSS nurse follow up Clinic review Horizons etc
Getting it right from the beginning • CHSS FAST campaign due to begin in October • May have implications for patient numbers and review in A&E • GPs need to be aware of stroke symptoms and thrombolysis service • NHS24 are reviewing stroke protocol
IV thrombolysis Outcome for placebo, rt-PA in clinical trials and SITS-MOST SITS is a register of thrombolysis in clinical practice Proportion of patients with good outcomes (0-2) is higher in SITS group than placebo group from clinical trials (Just in case you need evidence!)
Outcome following rt-PA Earlier is better
Assessment of Stroke Patients in A&E Patients who have a neurological deficit may be suitable for thrombolysis if they are scanned within 4.5 hours of symptom onset. Has the patient got an ongoing neurological deficit? e.g. Facial weakness Limb weakness Speech disturbance (dysphasia or dysarthria) Hemianopia Time is brain! NO YES If resolved anterior circulation symptoms and/or AF, discuss with stroke bleep holder re urgent investigation. Refer other patients to neurovascular clinic (fax letter to 559506) Known time since onset <4.5 hours? No contraindication to thrombolysis?** Time since onset >4.5 hours or unknown? Arrange urgent CT scan then contact stroke bleep via switchboard (If no response, contact Dr Macleod on page 3132, tel 645250 or 07771631243) Contact stroke team to arrange admission **Contraindications to thrombolysis Minor neurological deficit or symptoms rapidly improving before start of infusion. Symptoms of ischaemic attack began more than 4 hours prior to referral, or when time of symptom onset is unknown. Severe stroke as assessed clinically (e.g. NIHSS>25) and/or by appropriate imaging techniques. Seizure at onset of stroke. Symptoms suggestive of subarachnoid haemorrhage, even if the CT-scan is normal. On warfarin therapy, or administration of heparin within the previous 48 hours and a thromboplastin time exceeding the upper limit of normal for laboratory. Patients with any history of prior stroke and concomitant diabetes. Prior stroke within the last 3 months. Platelet count of below 100,000/mm3 (if available). Systolic blood pressure >185 mmHg or diastolic blood pressure >110 mmHg, or aggressive management (IV medication) necessary to reduce BP to these limits. Blood glucose <3 or > 20 mmol/L. Known haemorrhagic diathesis, manifest or recent severe or dangerous bleeding, known history of or suspected intracranial haemorrhage.
Thrombolysis in Grampian • Approx 20 patients so far this year • Still only about 2-3% of patients • Recent audit suggested most appropriate patients offered therapy (i.e. most are arriving too late)
Example patient 1 • 54 year old off shore worker from Kilmarnock • Walking along Market St prior to joining ship • Developed dense left sided weakness • Arrived A&E within thirty minutes • Reviewed within one hour • CT scan and thrombolysed within 1 ½ hours • Initial dramatic improvement, but symptoms returned at approx 1 hr after thrombolysis • Internal capsule infarct on repeat scan at 24 hours • Good progress with physiotherapy/OT • Transferred back to Kilmarnock for rehab
Example patient 2 • 71 year old • History of HBP, IHD • 0530 at Montrose harbour, about to go prawn fishing with brother • Hauling creels • Suddenly collapsed: right sided weakness and aphasia by arrival in A&E at 0700 • Reviewed 0720 • CT scan showed L intracerebral bleed • Slow progress, still on ward three weeks later awaiting transfer to slow stream rehab.
Even if not suitable for thrombolysis……… • Early review of patients is associated with improved outcomes • Early scanning • Immediate management protocol • Secondary prevention protocol • Early carotid intervention
Why are we proud of the ASU? We are a TEAM!! Social work CHSS nurses Links with Woodend Vascular surgery Speech & Language Database coordinator Patient Nursing staff Medical staff Dietician Radiology Research staff Physiotherapy Neuropsychology Mobile stroke team Occupational therapy
How can we make the pathway better? • All appropriate patients coming to ASU • (would allow redeployment of MST) • Quicker ‘run off’ to Wards 12, 6 and interim care • Improve links with Radiology (new CT scanner in March 08 will allow perfusion CT/angiography which aids in diagnosis and decision making) • Implement SIGN guidelines • Continue to aim towards QIS standards • Development of early supported discharge team