Download
1 / 1
10 likes | 152 Views
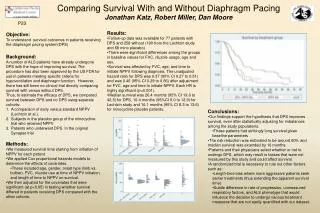
Comparing Survival With and Without Diaphragm Pacing Jonathan Katz, Robert Miller, Dan Moore. P23. Results: Follow-up data was available for 77 patients with DPS and 258 without (190 from the Lechtzin study and 68 mino placebo).

E N D
Comparing Survival With and Without Diaphragm PacingJonathan Katz, Robert Miller, Dan Moore P23 • Results: • Follow-up data was available for 77 patients with DPS and 258 without (190 from the Lechtzin study and 68 mino placebo). • There were significant differences among the groups in baseline values for FVC, riluzole usage, age and sex. • Survival was affected by FVC, age, and time to initiate NPPV following diagnosis. The unadjusted hazard ratio for DPS was 0.37 (95% CI 0.27 to 0.51) and was 0.40 (95% CI 0.29 to 0.56) after adjustment for FVC, age and time to initiate NPPV. Each HR is highly significant (p<0.001). • Median survival was 26.4 months (95% CI 19.6 to 42.5) for DPS, 10.4 months (95%CI 9.0 to 12.9) for Lechtzin study and 10.1 months (95% CI 8.3 to 13.6) for minocycline placebo patients. Objective: To understand survival outcomes in patients receiving the diaphragm pacing system(DPS) • Background: • A number of ALS patients have already undergone DPS with the hope of improving survival. The procedure has also been approved by the US FDA for use in patients meeting specific criteria for hypoventilation and diaphragm function. However, there has still been no clinical trial directly comparing survival with versus without DPS. • Thus, to estimate the efficacy of DPS, we compared survival between DPS and no DPS using separate cohorts: • A comparison of early versus standard NPPV (Lechtzin et al.), • Subjects in the placebo group of the minocycline trial who received NPPV • Patients who underwent DPS. In the original Synapse trial • Conclusions: • Our findings support the hypothesis that DPS improves survival, even after statistically adjusting for imbalances among the study populations. • These patients had strikingly long survival given baseline parameters • The risk reduction was estimated to be around 60% and median survival was extended by 16 months. • Patients and their physicians select whether or not to undergo DPS, which may result in biases that were not measured by this study and could affect survival. • A randomized trial is necessary to rule out other factors such as: • Length-time bias where more aggressive patients seek earlier treatments (thus extending the apparent survival time) • Subtle difference in rate of progression, unmeasured respiratory factors, and ALS phenotype that would influence the decision to undergo various treatment measures that are not easily quantified with our dataset. • Methods: • We measured survival time starting from initiation of NPPV for each patient • We applied Cox proportional hazards models to determine the effects of covariates. • These included age, gender, onset type (limb vs. bulbar), FVC, riluzole use at time of NPPV initiation, and length of time to NPPV on survival. • We then adjusted for the covariates that were significant (at p<0.05) in testing whether survival differed in patients receiving DPS compared with the other cohorts.