Download
1 / 51
520 likes | 762 Views
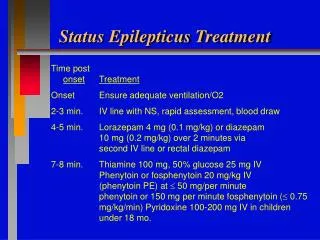
The Practical Management of Status Epilepticus. David Y. Gosal, Neuro SpR, Manchester Neurosciences Centre. Before I commence….

E N D
The Practical Management of Status Epilepticus David Y. Gosal, Neuro SpR, Manchester Neurosciences Centre
Before I commence… • The following is a synthesis of best available published information, national and local practice guidelines amongst Neurologists/Intensivists, and finally personal practice. • All criticism welcome.
How To Define Status? • 1981, ILAE (International League against Epilepsy) “a seizure that persists for a sufficient length of time or is repeated frequently enough that recovery between attacks does not occur”
How To Define Status? • More recent publications “A condition in which epileptic activity persists for 30 min or more” • Based on primate models of the estimated duration necessary to cause neuronal injury.
But • This is not practical operational definition. • Longer periods with uncontrolled seizure activity, more likely to develop a RSE syndrome. • More practical guidelines needed to draw that arbitrary ‘line in sand’, beyond which substantial risk of developing clinical SE exists.
Operational Definition “Continuous seizures lasting at least 5 minutes or two or more discrete seizures between which there is an incomplete recovery of consciousness.”
Compensated Decompensation
Premonitory Stage (pre-status) • Build up of seizure activity • Increasing frequency and / or severity of events. • Commonly 2mg-4mg lorazepam given. • A proportion of cases of early status can be terminated.
Confident diagnosis GTC status not always possible • Pseudoseizures • Minor motor features • Subtle SE (Electromechanical dissociation) small amplitude twitching movements. occasionally quiet. • CPSE
Pseudoseizures • Genuine and factitious seizures commonly occur in same individual. • 80% patients with NEAD are on anticonvulsants. • 1/3 patients present with ‘status’. • 2/3 positive motor attacks. • If treated as per status are highly likely to end up on anaesthetic agents. • Can appear focal onset, bite tongue, become incontinent.
Pseudoseizures: clinical features • Difficult, share many common characteristics. • Tremor like asynchronous waxing and waning asynchronous movement. • Thrashing limbs. • Pelvic thrusting. • Back arching. • Unresponsive , resists eye opening, versive eye movement to confrontation, strong stimuli. • Fever, tachycardia, leucocytosis, acidosis non-specific and late.
Could this be pseudoseizure activity? • On balance, where there exists doubt, so long as possibility of functional attacks have been considered but felt less likely (and documented as such), prompt treatment is best.
Basic investigation and general medical management • ABC. • Usual bloods. • Serum drug levels: CBZ, Phenytoin, Valproate. • Store 20mls of blood, and urine for toxicology if no obvious aetiological cause.
Initial treatment (Early Status 10-30min) • One area where some good class I evidence exists. • Three RCTs.
Pre-hospital treatment by paramedics. 2mg lorazepam, or 5mg diazepam Placebo Repeated dose after 4min if still actively seizing Lorazepam terminated 59.1% Diazepam 42.6% Placebo 21%
384 patients 0.1mg/kg lorazepam 15mg/kg phenobarbital 0.15mg/kg diazepam / 18mg/kg phenytoin 18mg/kg phenytoin
Duration of status and response to initial therapies Lowenstein et al., Neurology 1993;43:483
Initial anti-epileptic drug treatment (0-60min) • Lorazepam is benzodiazepine of choice. • Smaller volume of distribution • Longer therapeutic half-life. Anti-seizure effect 12hrs. • Relatively fast onset action • Previous rectal diazepam does not preclude its use • 2mg aliquots upto a max dose of 8mg in total • Diazepam • More lipid soluble • Shorter half-life. Anti-seizure effect 15-30min. • Repeated dosing • Faster onset ?Respiratory compromise -- Consider lignocaine / valproate
Initial anti-epileptic drug treatment (0-60min) • I personally follow on with second-line agent in any individual with early status, irregardless of seizure termination with benzodiazepines. • Phenytoin / Phenobarbitone most logical choices. • No evidence currently to choose between agents in terms of efficacy, although in general phenobarbitone is quicker in onset. • Phenytoin more widely accepted and used than phenobarbitone possibly because historically, oral phenytoin was preferred to phenobarbitone as maintenance therapy.
Initial anti-epileptic drug treatment: Sodium Valproate • If worried re arrhythmias, hypotension, sedation, can use valproate. • Has been reported to be effective in GTCSE. • Efficacy rates 63% in one study. • Loading dose 25-45mg/kg. Rate 200-500mg/min. • Continuous infusion rate upto 6mg/min.
384 patients 0.1mg/kg lorazepam 15mg/kg phenobarbital 0.15mg/kg diazepam / 18mg/kg phenytoin 18mg/kg phenytoin
Initial anti-epileptic drug treatment: Sodium Valproate • If worried re arrhythmias, hypotension, sedation, can use valproate. • Has been reported to be effective in GTCSE. • Efficacy rates 63% in one study. • Loading dose 25-45mg/kg. Rate 200-500mg/min. • Continuous infusion rate upto 6mg/min.
Phenytoin • Common problem is that about 70% patients admitted to ITU are given an inadequate loading dose. • I normally give a dose of 15mg/kg at a rate of 50mg/min in young, 20-30mg/min in elderly. • Risk bradycardia secondary to drug, and hypotension secondary to glycol additives. • A further 5mg/kg given almost immediately afterwards if no response to initial dose. • Can give upto 30mg/kg., before consideration anaesthesia. • Cardiac monitoring necessary..unnecessary delays. • 15-20minutes at least to take effect.
Phenytoin • If already on phenytoin, give 10mg/kg, and request urgent levels. • Must be aggressive with dosing, and even if responds to initial dose, should aim for high normal levels. Range 40-80 micromoles/litre. • Request serum phenytoin level 1/2hr to 1 hr after loading dose, and keep giving iv aliquots, with levels after each dose until desired range. • In general for micromoles/l, for every 4 micromoles/l off desired target, give 1mg/kg.
Phenytoin • Non-linear elimination kinetics because capable of saturating metabolising enzyme. • In general 20mg/kg usually saturates. • Predominately protein bound. In hypoalbuminaemic states can be clinically toxic with apparently normal total serum levels. Adjusted Phenytoin = Measured total conc. (0.2 x albumin) + 0.1
Refractory Status (60min onwards) • No accepted definition. • 30-50% patients fail initial benzo / phenytoin Rx. • Expert consensus and all current guidelines advise that by this stage patient should be transferred to ITU for general anaesthesia. • Urgently suppress seizures (Time is brain) • Manage systemic adverse effects • Find possible aetiology • SE becomes more refractory with time • RSE Mortality 20%
Mortality 30% Compensated Decompensation
Refractory Status (60min onwards) • No accepted definition. • 30-50% patients fail initial benzo / phenytoin Rx. • Expert consensus and all current guidelines advise that by this stage patient should be transferred to ITU for general anaesthesia. • Suppress seizures • Manage systemic adverse effects • Find possible aetiology • SE becomes more refractory with time • RSE Mortality 20%
But, in practice • 60% European Neurologists, epileptologists, intensivists use third anti-epileptic agent. • (43% US) • Some evidence to show that 50% refractory cases successfully treated. • ?but at what cost.
Anaesthetic agents • Choice of agent • What depth of anaesthesia
Treatment of Refractory Status Epilepticus with Pentobarbital, Propofol, or Midazolam: A Systematic review Jan Claassen et al., Epilepsia, 43(2);146-153, 2002 193 patients, 28 trials.
Propofol in the treatment of refractory status epilepticus Parviainen I et al., Intensive Care Med (2006) 32:1075 • 10 patients with refractory SE. • Terminated seizure activity in all initially. • Quality of burst suppression unsatisfactory. • Incremental doses of propofol needed. • Most needed noradrenaline. • Need continuous EEG monitoring. • Stepwise weaning, risk of emergent seizure activity. Reduction 5% infusion rate/hr over 24hours. • Weaning time from ventilator 50% quicker than thiopentone.
Similar to propofol, effectively terminated seizures. • Easier to attain and keep burst suppression. • Doses needed higher than generally recommended. • Recovery from anaesthesia prolonged • ---most had co-morbid conditions. • Most ended up with RTI. • Theoretical advantage of being neuroprotective by dose-dependently reducing cerebral metabolic rate and 02 comsumption.
127 patients with status epilepticus. • 47 patients with RSE of various aetiologies. • 2/3 “burst suppression”. • Incidence of potentially serious / fatal aetiologies same in both groups. • “Outcome was independent of the specific coma-inducing agents used and the extent of EEG burst suppression, suggesting that the underlying cause represents the main determinant”. • Mortality 23% RSE, 8% SE • Baseline 31% RSE, 50% SE
Conclusions in RSE • Evidence for treatment poor and based on retrospective studies. • More important to initiate anaesthesia with undue delay, rather than argue over pros and cons of any particular treatment. • Continuous monitoring until electrographic seizures abolished, and at least daily monitoring is required in all cases of RSE is a minimum. • Is burst suppression really necessary? Prospective trial • How long anaesthesia should be administered is unclear, and probably depends on underlying aetiology. • Barbituates have someadvantages over other agents, but at expense of respiratory complications and prolonged ITU stay. • Prognosis ultimately depends on aetiology.
What if nothing works? • Repeated failed attempts at withdrawal anaesthesia. • Even with known epilepsy, should have MRI and CSF as a minimum. • Serum amticonvulsant levels. • Alternative anti-epileptics… • iv valproate worth a go • Leviteracetam • Topiramate • Anoxic / metabolic brain damage..Post-anoxic myoclonus? • Longer and deeper anaesthesia.
Prognosis • Mortality and morbidity severely influenced by underlying aetiology. Cannot give reliable figures for condition itself. • Mortality 20% • Morbidity; high risk recurrent seizures, cognitive deficits, and future episodes • Many aetiological causes, useful to divide into acute and chronic processes.
Acute processes Stroke Metabolic disturbances CNS infection Trauma Drug Toxicity Hypoxia Difficult to manage Higher mortality Chronic processes Pre-existing epilepsy Ethanol abuse Old CVA Relatively long-standing tumours
Other forms of status • Non-convulsive status epilepticus (NCSE). • Myoclonic status. • Focal motor status
Non-convulsive status epilepticus • Absense Status • Rare • Primary generalised epilepsy • Learning disabled • Profound stupor • Occur after tonic-clonic seizure / GTCSstatus • Eyelid / facial myoclonia • Little evidence that it is harmful in itself • Iv valproate, or iv benzodiazepines
Non-convulsive status epilepticus • Complex partial status epilepticus • Much more prevalent • Elderly • Vastly under-diagnosed • Confused…profound stupor • Focal motor phenomenon • Fluctuating symptoms • Level of consciousness can be occasionally significantly impaired…iv phenytoin, and occasionally will need anaesthesia • Quite refractory to treatment. • Unsure how aggressively to treat..individualistic.
Non-convulsive status epilepticus • Husain et al, 2003, JNNP,74,189-91 • Altered consciouness / mental state • Remote risk factor seizure eg previous stroke • Ocular movement abnormality • 100% predictive value
Myoclonic status • Usually seen with the primary epilepsy syndromes. • Can be a sign of impending tonic-clonic status. • IV benzodiazepine • IV valproate
Focal motor status • Epilepsia partialis continua (EPC).
Conclusions • Serious medical condition with high mortality rate. • Relative dearth of evidence on how to treat condition. • Despite this, good practical guidelines exist. • Pick your drugs, know them well, and use enough. • Ask for specialist help early. • Prognosis depends on aetiology, delay in initiation of appropriate treatment, and usual co-morbid factors.