Status Epilepticus
Status Epilepticus. Dr. Esther Tsang Sept 2011. Case 1. A 16 year old young boy was brought in at 2am by his friends due to a ‘seizure’. They came from a night club and according to his friends, he had a mild fever in the morning.

Status Epilepticus
E N D
Presentation Transcript
Status Epilepticus Dr. Esther Tsang Sept 2011
Case 1 • A 16 year old young boy was brought in at 2am by his friends due to a ‘seizure’. • They came from a night club and according to his friends, he had a mild fever in the morning. • What points in the history should you ask for to support a diagnosis of a seizure? • What other history would you ask for based on this background history? • What could be the possible causes of seizure in this gentleman?
When you examine him, he appears somnolent. • He is arousable, able to say his name, confused, obeys commands, moving all four limbs. • What is his GCS? • As you examine him, you notice that his breath reeks of alcohol. Then, he looses consciousness, has jerky movements of his upper limbs and lower limbs, and turns blue.
What do you do now? • What are your options if you are unable to secure IV access?
The seizure self aborts after 2 mins. He regains his colour and breathing returns to normal. • You note that his neck is rather stiff. • What would be your working diagnosis now? • What investigations would you want to order and why?
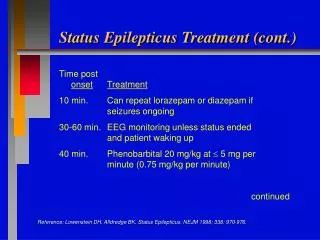
As you are writing up the orders, he has another seizure. • This time, he does not wake up after 5 mins. • His breathing is laboured. • The medical officer in casualty tells you that his SpO2 was 88%, BP 130/70 mm Hg, HR 120, T 38°C. • So, is this status epilepticus? • How do you define status epilepticus?
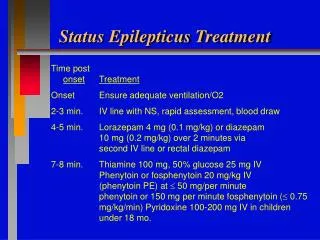
When do you decide to intubate this patient and why? • How would you manage this patient now? • What medications should you order and how to you start it? • What are the second line medications should the first one fail o control the seizures? • The casualty MO suggests starting him on IV Thiamine prior to a dextrose drip. Do you think this is wise? Why?
Your medications fail to control the seizures, and he develops another 2 seizures. You decide to intubate him and refer him to ICU. • Describe what medications you would give prior to intubation. • Describe the methods used to place the ETT correctly.
The patient is then sent to ICU. • The ICU MO wants to know how the anti-epileptics should be served? • Are there any drug interactions between the antiepileptics?
After being treated 5 days in the ICU, your patient is now awake, and alert. He is ready to be discharged to the general ward. • During your ward rounds, he asks you the following questions. • Does he have to take the anti-epileptic medications permanently? • What are the side effects of the medications? • What are the symptoms of toxicity of the medications? • Can he drive?