Download
1 / 18
180 likes | 265 Views
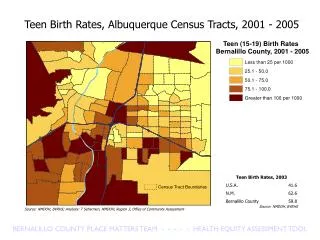
An Assessment of First Dental Visits Between Birth and the 1 st Year, Utah 2001-2005. Shaheen Hossain, PhD Karen L. Zinner, MPH Peggy A. Bowman RDH, BA Steven Steed, DDS Gail Rapp, MS 11th Annual Maternal and Child Health Epidemiology Conference, Miami 2005. Presentation outline. Policy.

E N D
An Assessment of First Dental Visits Between Birth and the 1st Year, Utah 2001-2005 Shaheen Hossain, PhD Karen L. Zinner, MPH Peggy A. Bowman RDH, BA Steven Steed, DDS Gail Rapp, MS 11th Annual Maternal and Child Health Epidemiology Conference, Miami 2005
Presentation outline Policy Study Intervention Follow-up AAPD (1986) and ADA (2000) recommend first dental visit by 1st year of age UDOH conducts a study (2001) to determine compliance with the new policies Utah implements several interventions during 2002 - 2005 UDOH conducts a follow-up survey (2005) to compare with 2001 baseline data AAPD - American Association of Pediatric Dentists ADA - American Dental Association UDOH - Utah Department of Health
Prevalence of dental caries • Dental caries comprise the single most common chronic disease affecting children in the U.S. • Rate for caries increases with age* • 2 - 4 yrs 18% • 6 - 8 yrs 52% • 15 yrs 61% • 17 yrs 78% • ≥18 yrs 85% • Low income and minority children have a higher risk of developing caries in primary teeth * HP 2010 baseline data for objective #21a-c, and US Department of Health and Human Services. Oral Health in America: A Report of the Surgeon General; 2000
Impact of untreated dental caries • Average cost for treatment of early childhood caries ranges from $1,500 to $2,000* per child • Missed school days • Decreased school performance • Impaired speech development • Poor self-esteem * US Department of Health and Human Services. Oral Health in America: A Report of the Surgeon General; 2000
Guideline on infant oral health care • Previous recommendations suggested that a child have an initial dental visit at age 3 • AAPD (1986) implemented a policy recommending an initial dental visit within 6 months of the eruption of a child’s first tooth and no later than 12 months of age • ADA (2000) reinforced AAPD’s policy and recommended that a child’s first dental visit occur by age one
2001 Utah dentist survey • Purpose: Utah Oral Health Program (OHP) surveyed licensed general and pediatric dentists in Utah to assess the earliest age which they saw children • Time Period: Oct 2001 – Jan 2002 • Surveys mailed: 1,339 • Response rate: 63% (adjusted 61%, n=792)
Results of 2001 Utah dentist survey Earliest age dentists see children, Utah 2001 Most frequent response
UDOH activities during 2002-2005 • Training and education (e.g. Presented at Annual American Dental Hygienists Association conference, Pediatric Grand Rounds, Utah local health departments, Utah Dental Association Annual conference, Telehealth broadcast and WIC conference) • Development of educational materials (e.g. Articles in Utah WIC program newsletter, Head Start newsletter, and Baby Your Baby) • Collaboration with Utah Dental Association (e.g. UDOH worked together with dental health care professionals to promote early dental visits, and UDA visits to local dental societies) • Held Oral Health Summit (Inspire Utahns to take an active role in enhancing oral and general health for all children in Utah)
New infant oral health care guidelines • American Academy of Pediatrics (2003*) recommends children should receive oral health evaluation by 6 months of age by a pediatrician or other qualified pediatric health care professional • Oral health risk assessment should include: • Assess mother’s oral health • Assess oral health risk of children • Perform oral health examination and recognize risk of caries • Assess child’s exposure to fluoride • Educate parents on oral hygiene and diet • Make referral to dental home if necessary * Oral Health Risk Assessment Timing and Establishment of the Dental Home, Pediatrics. 2003. Vol. 111
Surgeon General’s Call to Action 2003 • The goals of this Call to Action were: • To promote oral health • To improve quality of life • To eliminate oral health disparities • Call to Action identified 5 action areas: • Change perceptions of oral health • Replicate effective programs and proven efforts • Build the science base • Increase oral health workforce diversity, capacity and flexibility • Increase collaborations • “No one should suffer from oral diseases that can be effectively prevented and treated”
2005 Utah dentist survey • Purpose: Determine if there had been a change in the practice of seeing young children • Time Period: Feb 2005 – Mar 2005 • Surveys mailed: 1,112 • Response rate: 58% (adjusted 57%, n = 605)
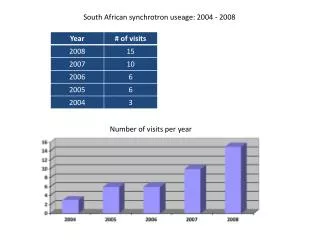
Results of 2005 Utah dentist survey Earliest age dentists see children, Utah 2005 Age 0-1 Yrs 2 Yrs 3 Yrs 4 Yrs 5-6 Yrs Percentage 23.8% 35.6% 36.0% 3.3% 1.2%
Comparison of 2001 and 2005 surveys Earliest age dentists see children, Utah 2001 and 2005 * z-test proportional difference using SAS 9.1
Survey comments • Most general practice dentists who commented said they felt pediatric dentists were better suited to treat young children (26.8%) • Additional reasons for not treating children at an early age • Had an adequate referral source (13.0%) • Practice was not geared to treat young children (8.0%)
Limitations • Limited demographic data was obtained in the surveys • Non-respondents may have different experiences and opinions regarding practice pattern (43% non-response rate)
Conclusions and implications • Preventing dental decay should begin with pregnant women and continue with the mother and child • Dentists need to be more informed regarding current oral health policies • Pediatricians’ roles need to be expanded to include promotion of children’s oral health • Public health professionals who serve mothers and infants need to provide education to parents on the etiology and prevention of caries
Contact information Oral Health Program Utah Department of Health 801-538-9177 http://health.utah.gov/oralhealth/ Gail Rapp, M.S. Oral Health Program Manager gailrapp@utah.gov Steven Steed, D.D.S. Utah State Dental Director stevensteed@utah.gov