Download
1 / 59
590 likes | 614 Views
This overview provides information on the causes, symptoms, and treatment of meningitis, an inflammation of the meninges. It includes details on different types, risk factors, pathogenesis, diagnostic tests, and management options.

E N D
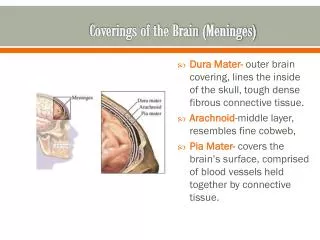
Meningitis inflammation of the meninges • Inflammation of the brain cortex is called encephalitis • Meningismus refers to meningeal irritation not due to CNS infection
Meningitis -overview AETIOLOGY < 5years Haemophilus influenzae Type B Streptococcus pneumoniae Neisseria Meningitidis >5years Neisseria Meningitidis Haemophilus influenzae Type B Streptococcus pneumoniae • Neonatal period Group B streptococcus E.Coli Listeria Monocytogen
Risk factors • GROMAP Genetic susceptibility Race (black race) Overcrowding Male gender Young Age Poverty
Route of infection • Haematogenous spread • Direct contiguous spread Acquired defect-trauma with basal skull fracture Congenital defects: meningomyelocele Lumbaosacraldural sinus cribriform plate (roof of the nose) stapedial foot plate(Middle ear) inner ear-oval window, internal auditory canal, cochler aqueduct
Pathogenesis • Immune system activation with subsequent cytokine production • Increased BBB permeability • Altered cerebral blood flow • Increased reactive oxygen species • Leucocytes adherence to capillary endothelium
Pathogenesis CT…. • The final 4 pathological processes will lead to • Neuronal death • Increased ICP • Cerebral oedema
Q &A Concerning meningitis Symptoms and signs are specific during the neonatal period Children with anatomic defect or functional asplenia have infection rate higher than healthy children N. Meningitidis has 5 major serogroups A, B, C, Y and W135, epidermics in Africa is assted with serogroup A and C Preceding history of upper respiratory tract infection is sacrosanct Inflammation of the spinal nerves and roots produces meningeal signs Streptococcal meningitis has the highest mortality rate while, H. influenzae has the lowest mortality rate
Q &A The seizure is caused by cerebritis, infarction and electrolyte disturbance Hypoglycorrhachia is attributable to decreased glucose transport by the cerebral tissue Raised CSF protein is as a result of increased vascular permeability of BBB and the loss of albumin-rich fluid from the capillaries and vein traversing the subdural space Blood culture should performed in all patient with suspected meningitis-positive in 80-90% of cases. The classical CSF finding in Bacterial meningitis is increased WBC, increased protein and reduced CSF glucose
pleocytosis, hypoglycorrhachia and elevated protein is the usual CSF findings in bacteria meningitis. • Duration of treatment for bacteria meningitis Strep pneumonia is 10-14days H. influenzae is 7 -10days N.meningitis is 5-7days gram negatives bacillary meningitis is treated for 3weeks
L4 /L5 is used for children while L3/L4 is used for Adult b/c spinal cord ends at L1. • Contraindication to lumbar puncture • Evidenced of raised ICP • Severe cardiopulmonary compromise • Infection at the LP site • Thrombocytopenia is a relative contraindication
The CSF should be sterile within 24-48hr of initiation of appropriate antibiotic therapy. • what are the causes of CSF xanthochromia • Traumatic lumber puncture • Subarachnoid haemorrhage • Hyperbilirubinaemia • Markedly elevated CSF protein
Evidenced of raised ICP and severe cardiopulmonary compromise are contraindications for LP • Site for LP is L3/L4 or L4/L5 • Xanthochromia is pathognomonic for subarachnoid haemorrhage • Viral meningitis is usually less severe than bacteria meningitis • All patient with bacterial meningitis shd be assessed for hearing or visual deficit before discharge.
Concerning febrile convulsion • convulsion in child age 6month-5yrs • convulsion occurs at the peak of fever • it is due to convulsion of extra cranial origin • Complex febrile convulsion has a better prognosis than simple febrile convulsion • There is a genetic predisposition to febrile convulsion-inheritance is autosomal dominant • Lumber puncture is indicated in infants < 6momths
There is 1-2% risk of developing epilepsy after simple febrile seizure • The risk of developing epilepsy is 4-12% after complex FS • EEG is indicated after febrile seizure
What are the risk factors for recurrence of febrile seizures • Major risk factors • Age <1yr • Duration of fever < 24hrs • Fever of 38-390c
Minor risk factors • Family hx of FS • Family hx of epilepsy • Complex febrile seizure • Male gender • Day care • Low serum sodium at time of presentation
Identify the abnormalities in the blood filmof 9months old child who presented with unconsolable cry and sever pallor
What is you your tentative diagnosis • What is the confirmatory diagnostic investigations • List the major crisis in this condition • List 5 acute complications of SCA • List 5 chronic complications of SCA • Give 5 reasons why they are prone to infections and what type of infection are they prone to ? • List the recommended vaccines for the SCA • List the various factor associated with SCA severity
Overview of SCD • SCD is a systemic disorder caused by mutation in the gene encoding the beta chain of Haemoglobin.This mutation leads to the production of sickle haemoglobin (Hbs) • Hbs is the result of a single base pair change(point mutation), thymine replaces adenine at the 6th codon of the beta globin gene. This change result in the encoding of valine instead of glutamine in the 6th position of the beta globin molecule
What is Sickle cell disease What is Sickle cell anaemia What is sickle cell trait What is the inheritance pattern of SCD
The inheritance of two abnormal haemoglobin genes, at least one of which is a sickle haemoglobin gene (Hbs) is called sickle cell disease. • The inheritance of two sickle haemoglobin genes give rise to sickle cell anaemia, (Hbss) Sickle cell anaemia is the most common and most severe of the sickle cell disease • Other sickle cell disease include: HbSC, HbBetathalasaemia +, HbBetathalasaemia zero, HbSD, HbSE, HbSOArab
The inheritance of one normal haemoglobin gene with a sickle haemoglobin gene result in sickle cell trait. Sickle cell trait is not considered as part of sickle cell disease spectrum
Sickle cell haplotypes • Saudi Arabian/Indian • Senegal • Benin • Bantu • Cameroon
Haplotyping has clinical significance. • Sickle cell anaemic patient with Senegal or Saudi Arabia/india haplotype tend to have mild clinic course as a result of high HbF levels seen in such individual
PATHOPHYSIOLOGY • 1. Sickle haemoglobin polymerization • 2. Increased adhesion of sickle RBC to endothelium • 3. Haemolysis • 4. free radical
CRISIS IN SCA 1.Vaso-occlusive crisis 2.Hyperhaemolytic crisis 3.Sequestration crisis 4.Aplastic crisis
Acute complications of SCA • Vaso occlusive crisis • Acute chest syndrome • Cerebrovascular accident • Anaemic crisis(Aplastic, acute splenic sequestration and hyperhaemolytic) • Priapism • Bacteria sepsis
Chronic complication • Silent stroke • Sickle cell nephropathy • Sickle cell retinopathy • Avascular necrosis of the femoral head • Delayed onset of puberty • Leg ulcer • Pulmonary hypertension • Sensorineural hearing loss
SCA and infection • SCA are prone to infection by encapsulated organisms Streptococcus pneumoniae Haemophilusinflunzae type b Neissaria meningitidis Salmonella sppetc Fever in a child with SCA is a medical emergency requiring prompt medical evaluation and delivery of antibiotics
Factors responsible for increased susceptibility to infection (SCA) • Splenic hypofunction • Complement alternate pathway impairment-defective opsonization • Abnormal leucocyte phagocytic function • Elevated serum iron • Recurrent vaso-occlusion resulting in necrotic tissue which may habour bacteria • Micronutrient deficiencies e.g zinc
Immunization for SCA Immunization to protect against encapsulated organisms 1.Pneumococcal vaccine 2 .Haemophilus influenzae type b (Hib)vaccine 3. Meningococcal vaccine 4. Samonella vaccine
Factors that influences the severity of clinical manifestation • 1. fetal haemoglobin levels- HbSS with high HbF have milder disease course. • 2. haplotype- HbSS Patients with Bantu haplotype have worst disease course • 3.Co- existent apha-thalassaemia-less severity • 4.HbSS with associated other enzyme deficiencies e.g G-6-P-D –more prone to repeated haemolytic crisis • 5.Environmental factors
DEFINITONS OF TERMS • MALNUTRITION is defined as cellular imbalance between supply of nutrient and energy and the body’s demand for them to ensure growth and maintenance of specific function • SEVER ACUTE MALNUTRITION is defined as severe wasting and/or bilateral oedema.
What is severe wasting • Severe wasting is extreme thinness diagnosed by weight for length(or height) below -3SD of the WHO child growth chart. • In children ages 6-59months, a MUAC <115mm also denote extreme thinnes
Types of malnutrition • PRIMARY MALNUTRITION- caused by deficiency of food availability • SECONDARY MALNUTRITION-Food is available but the body cannot assimilate it for one reason or the other
CLASSIFICATION OF MALNUTRITION • WHO Classification Weight for height evaluate wasting=Acute malnutrition. WFH <-3SD= Severe wasting Height for Age-evaluate stunting=chronic malnutrition HFA <-3SD= severe stunting
Modified welcome classification( %weight for Age plus or minus oedema) Oedema absent oedema present <60% marasmus marasmuskwas 60-80% underweight kwashiokor >80 Normal Overweight kwas
Gomez classification • Waterlow classification
AETIOLOGY OF MALNUTRITION • The cause of malnutrition- 3 levels • The immediate cause- inadequate intake and disease • The underlying cause- household food insecurity • The remote cause-natural diasters, conflicts, political/economic
Theories of malnutrition • The classical theory-oedema in kwas is due to hypoalbuminaemia, in marasmus the principal lacking factor is energy • Gopalan adaptation and dysadaptation theory • Golden’s theory of free radicals—causes cell membrane damage