Understanding Knee Anatomy and Functions by Dr. Michael P. Gillespie
1.18k likes | 1.38k Views
Explore the structure and biomechanics of the knee through detailed explanations by Dr. Michael P. Gillespie. Learn about bones, articulations, ligaments, and more in this comprehensive guide.

Understanding Knee Anatomy and Functions by Dr. Michael P. Gillespie
E N D
Presentation Transcript
KNEE Dr. Michael P. Gillespie
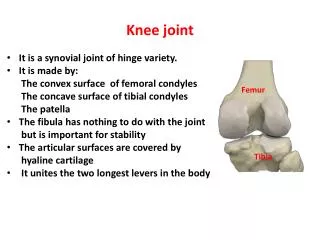
KNEE: GENERAL CONSIDERATIONS • The knee consists of lateral and medial compartments at the tibiofemoral joint and the patellofemoral joint. • Motion of the knee occurs in two planes: • Flexion and extension • Internal and external rotation • Two-thirds of the muscles that cross the knee also cross either the ankle or the hip. This creates a strong functional association within the joints of the lower limb. • Stability of the knee is based primarily on its soft-tissue constraints rather than on its bony configuration. Dr. Michael P. Gillespie
KNEE: BIOMECHANICAL FUNCTIONS • During the swing phase of walking, the knee flexes to shorten the functional length of the lower limb, thereby providing clearance of the foot from the ground. • During the stance phase, the knee remains slightly flexed allowing for shock absorption, conservation of energy, and transmission of forces through the lower limb. Dr. Michael P. Gillespie
OSTEOLOGY Dr. Michael P. Gillespie
BONES AND ARTICULATIONS OF THE KNEE Dr. Michael P. Gillespie
DISTAL FEMUR • At the distal end of the femur are the large lateral and medial condyles (Greek kondylos, knuckle). • Lateral and medial epicondyles project from each condyle. These serve as attachment sites for the collateral ligaments. • Intercondylar notch – passageway for the cruciate ligaments. • Femoral condyles fuse anteriorly to form the intercondylar (trochlear) groove. This groove articulates with the patella. • Lateral and medial facets – formed from the sloping sides of the intercondylar groove. • Lateral and Medial grooves are etched into the cartilage that covers the femoral condyles and the edge of the tibia articulates with these grooves. Dr. Michael P. Gillespie
OSTEOLOGIC FEATURES OF THE DISTAL FEMUR • Lateral and medial condyles • Lateral and medial epicondyles • Intercondylar notch • Intercondylar (trochlear) groove • Lateral and medial facets (for the patella) • Lateral and medial grooves (etched in the cartilage of the femoral condyles) • Popliteal surface Dr. Michael P. Gillespie
PATELLA, ARTICULAR SURFACES OF DISTAL FEMUR & PROXIMAL TIBIA Dr. Michael P. Gillespie
FIBULA • The fibular has no direct function at the knee; however, it splints the lateral side of the tibia and helps to maintain its alignment. • The head of the fibula is an attachment for biceps femoris and the lateral collateral ligament. • Proximal and distal tibiofibular joints attach the fibula to the tibia. Dr. Michael P. Gillespie
PROXIMAL TIBIA • The proximal end of the Tibia flares into medial and lateral condyles which articulate with the femur. • Tibial plateau – the superior surfaces of the condyles. • Intercondylar eminence – separates the articular surfaces of the proximal tibia. • Tibial tuberosity – anterior surface of the proximal shaft of the tibia. Attachment point for the quadriceps femoris, via the patellar tendon. • Soleal line – posterior aspect of tibia. Dr. Michael P. Gillespie
OSTEOLOGIC FEATURES OF THE PROXIMAL TIBIA AND FIBULA • Proximal Fibula • Head • Proximal Tibia • Medial and lateral condyles • Intercondylar eminence (with tubercles) • Anterior intercondylar area • Posterior intercondylar area • Tibial tuberosity • Soleal line Dr. Michael P. Gillespie
RIGHT DISTAL FEMUR, TIBIA, AND FIBULA Dr. Michael P. Gillespie
LATERAL VIEW RIGHT KNEE Dr. Michael P. Gillespie
PATELLA • The patella (Latin, “small plate”) is embedded within the quadriceps tendon. • The largest sesamoid bone in the body. • Part of the posterior surface articulates with the intercondylar groove of the femur. Dr. Michael P. Gillespie
OSTEOLOGIC FEATURES OF THE PATELLA • Base • Apex • Anterior surface • Posterior articular surface • Vertical ridge • Lateral, medial, and “odd” facets Dr. Michael P. Gillespie
PATELLA Dr. Michael P. Gillespie
ARTHROLOGY Dr. Michael P. Gillespie
GENERAL ANATOMIC AND ALIGNMENT CONSIDERATIONS • The shaft of the femur angles slightly medial due to the 125-degree angle of inclination of the proximal femur. • The proximal tibia is nearly horizontal. • Consequently, the knee forms an angle of about 170 to 175 degrees on the lateral side. The normal alignment is referred to as genu valgum. • Excessive genu valgum – a lateral angle less than 170 degrees or “knock-knee”. • Genu varum – a lateral angle that exceeds 180 degrees or “bow-leg”. Dr. Michael P. Gillespie
FRONTAL PLANE DEVIATIONS Dr. Michael P. Gillespie
CAPSULE AND REINFORCING LIGAMENTS • The fibrous capsule of the knee encloses the medial and lateral compartments of the tibiofemoral joint and patellofemoral joint. • Five regions of the capsule • Anterior capsule • Lateral capsule • Posterior capsule • Posterior-lateral capsule • Medial capsule Dr. Michael P. Gillespie
LIGAMENTS, FASCIA, AND MUSCLES THAT REINFORCE THE CAPSULE OF THE KNEE Dr. Michael P. Gillespie
ANTERIOR VIEW RIGHT KNEE: MUSCLES & CONNECTIVE TISSUES Dr. Michael P. Gillespie
LATERAL VIEW RIGHT KNEE: MUSCLES & CONNECTIVE TISSUES Dr. Michael P. Gillespie
POSTERIOR VIEW RIGHT KNEE: MUSCLES & CONNECTIVE TISSUES Dr. Michael P. Gillespie
MEDIAL VIEW RIGHT KNEE: MUSCLES & CONNECTIVE TISSUES Dr. Michael P. Gillespie
SYNOVIAL MEMBRANE, BURSAE, AND FAT PADS • The internal surface of the capsule is lined with a synovial membrane. • The knee has as many as 14 bursae. • These bursae form inter-tissue junctions involving tendon, ligament, skin, bone, capsule, and muscle. • Some bursae are extensions of the synovila membrane and others are formed external to the capsule. • Fat pads are often associated with the suprapatellar and deep infrapatellar bursae. Dr. Michael P. Gillespie
EXAMPLES OF BURSAE AT VARIOUS INTER-TISSUE JUNCTIONS Dr. Michael P. Gillespie
KNEE PLICAE • Plicae or synovial pleats appear as folds in the synovial membrane. • Plicae may reinforce the synovial membrane of the knee. • Three most common plicae: • Superior or suprapatellar plica • Inferior plica • Medial plica (goes by about 20 names including alar ligament, synovialis patellaris, and intra-articular medial band). • Plicae that are unusually large or thickened due to irritation or trauma can cause knee pain. • Inflammation of the medial plica may be confused with patellar tendonitis, torn medial meniscus, or patellofemoral pain. • Treatment includes: rest, anti-inflammatory agents, PT, and in severe cases arthroscopic resection. Dr. Michael P. Gillespie
TIBIOFEMORAL JOINT • Articulation between the large convex femoral condyles and the nearly flat and smaller tibial condyles. • The large articular surface area of the femoral condyles permits extensive knee motion in the sagittal plane. • There is NOT a tight bony fit at this joint. • Joint stability is provided by muscles, ligaments, capsule, menisci, and body weight. Dr. Michael P. Gillespie
SUPERIOR SURFACE OF TIBIA Dr. Michael P. Gillespie
POSTERIOR VIEW: DEEP STRUCTURES RIGHT KNEE Dr. Michael P. Gillespie
MENISCI: ANATOMIC CONSIDERATIONS • The medial and lateral menisci are crescent-shaped, fibrocartilaginous structures located within the knee joint. • They transform the articular surfaces of the tibia into shallow seats for the large femoral condyles. • Coronary (meniscotibial) ligaments anchor the external edge of each meniscus. • The transverse ligament connects the menisci anteriorly. • Several muscles have secondary attachments to the menisci. • Blood supply to the menisci is greatest near the peripheral border. The internal border is essentially avascular. Dr. Michael P. Gillespie
MENISCI: FUNCTIONAL CONSIDERATIONS • The menisci reduce compressive stress across the tibiofemoral joint. • They stabilize the joint during motion, lubricate the articular cartilage, provide proprioception, and help guide the knee’s arthrokinematics. • Compression forces at the knee reach 2.5 to 3 times the body weight when one is walking and over 4 times the body weight when one ascends stairs. • The menisci nearly triple the area of joint contact, thereby significantly reducing the pressure. • With every step, the menisci deform peripherally. • The compression force is absorbed as circumferential tension (hoop stress). Dr. Michael P. Gillespie
MENISCI: COMMON MECHANISMS OF INJURY • Tears of the meniscus are the most common injury of the knee. • Meniscal tears are often associated with a forceful, axial rotation of the femoral condyles over a partially flexed and weight-bearing knee. • The axial torsion within the compressed knee can pinch and dislodge the meniscus. • A dislodged or folded flap of meniscus (often referred to as a “bucket-handle tear”) can mechanically block knee movement. • The medial meniscus is injured twice as frequently as the lateral meniscus. Axial rotation with a valgus stress to the knee can cause this. Dr. Michael P. Gillespie
OSTEOKINEMATICS AT THE TIBIOFEMORAL JOINT • Two degrees of freedom: • Flexion & extension in the sagittal plane • Provided the knee is slightly flexed, internal and external rotation. Dr. Michael P. Gillespie
TIBIOFEMORAL JOINT: FLEXION AND EXTENSION • The healthy knee moves from 130 to 150 degrees of flexion to about 5 to 10 degrees beyond the 0-degree (straight) position. • The axis of rotation for flexion and extension is not fixed, but migrates within the femoral condyles. • The curved path of the axis is known as an “evolute”. • With maximal effort, internal torque varies across the range of motion. • External devices attached to the knee rotate about a fixed axis of rotation. A hinged orthosis can cause rubbing or abrasion against the skin. Goniometric measurements are more difficult. Place the device as close as possible to the “average” axis of rotation. Dr. Michael P. Gillespie
SAGITTAL PLANE MOTION AT THE KNEE Dr. Michael P. Gillespie
“THE EVOLUTE” Dr. Michael P. Gillespie
TIBIOFEMORAL JOINT: INTERNAL AND EXTERNAL (AXIAL) ROTATION • Internal and external rotation of the knee occurs about a vertical or longitudinal axis of rotation. • This motion is called axial rotation. • The freedom of axial rotation increases with greater knee flexion. • A knee flexed to 90 degrees can perform about 40 to 45 degrees of axial rotation. • External rotation generally exceeds internal rotation by a ratio of nearly 2:1. • Once the knee is in full extension, axial rotation is maximally restricted. • The naming of axial rotation is based on the position of the tibial tuberosity relative to the anterior distal femur. • External rotation of the knee is when the tibial tuberosity is located lateral to the anterior distal femur. • This does not stipulate whether the tibia or femur is the moving bone. Dr. Michael P. Gillespie
INTERNAL AND EXTERNAL (AXIAL) ROTATION OF THE RIGHT KNEE Dr. Michael P. Gillespie
ARTHROKINEMATICS AT THE TIBIOFEMORAL JOINT: EXTENSION OF THE KNEE • Tibial-on-femoral extension • The articular surface of the tibia rolls and slides anteriorly on the femoral condyles. • Femoral-on-tibial extension • Standing up from a deep squat position. • The femoral condyles simultaneously roll anterior and slide posterior on the articular surface of the tibia. Dr. Michael P. Gillespie
ARTHROKINEMATICS OF KNEE EXTENSION Dr. Michael P. Gillespie
ARTHROKINEMATICS AT THE TIBIOFEMORAL JOINT: “SCREW-HOME” ROTATION KNEE • Locking the knee in full extension requires about 10 degrees of external rotation. • It is referred to as “screw-home” rotation. • It is a conjunct rotation. It is mechanically linked to the flexion and extension kinematics and cannot be performed independently. • The combined external rotation and extension maximizes the overall contact area. This increases congruence and favors stability. Dr. Michael P. Gillespie
“SCREW-HOME” LOCKING MECHANISM Dr. Michael P. Gillespie
ARTHROKINEMATICS AT THE TIBIOFEMORAL JOINT: FLEXION OF THE KNEE • For a knee that is fully extended to be unlocked, it must first internally rotate slightly. • This internal rotation is achieved by the popliteus muscle. Dr. Michael P. Gillespie
ARTHROKINEMATICS AT THE TIBIOFEMORAL JOINT: INTERNAL AND EXTERNAL (AXIAL) ROTATION OF THE KNEE • The knee must be flexed to maximize independent axial rotation between the tibia and femur. • The arthrokinematics involve a spin between the menisci and the articular surfaces of the tibia and femur. Dr. Michael P. Gillespie
MEDIAL AND LATERAL COLLATERAL LIGAMENTS: ANATOMIC CONSIDERATIONS • The medial (tibial) collateral ligament (MCL) • A flat, broad structure that crosses the medial aspect of the joint. • Superficial part • Deep part • Attaches to the medial meniscus • The lateral (fibular) collateral ligament • A round, strong cord that runs nearly verticle between the lateral epicondyle of the femur and the head of the fibula • Does NOT attach to the lateral meniscus • The popliteus tendon crosses between these two structures Dr. Michael P. Gillespie
MEDIAL AND LATERAL COLLATERAL LIGAMENTS: FUNCTIONAL CONSIDERATIONS • The function of the collateral ligaments is to limit excessive knee motion within the frontal plane. • The MCL provides resistance against valgus (abduction) force. • The lateral collateral ligament provides resistance against varus (adduction) force. • Produce a general stabilizing tension for the knee throughout the sagittal plane range of motion. Dr. Michael P. Gillespie
ANTERIOR & POSTERIOR CRUCIATE LIGAMENTS: GENERAL CONSIDERATIONS • Cruciate, meaning cross-shaped, describes the spatial relation of the anterior and posterior cruciate ligaments as they cross within the intercondylar notch of the femur. • The cruciate ligaments are intracapsular and covered by extensive synovial lining. • Together, they resist the extremes of all knee movements. • The provide most of the resistance to anterior and posterior shear forces. • They contain mechanoreceptors and contribute to proprioceptive feedback. Dr. Michael P. Gillespie
ANTERIOR CRUCIATE LIGAMENT: ANATOMY AND FUNCTION • The anterior cruciate ligament (ACL) attaches along an impression on the anterior intercondylar area of the tibial plateau. • It runs obliquely in a posterior, superior, and lateral direction. • The fibers become increasingly taut as the knee approaches and reaches full extension. • The quadriceps is referred to as an “ACL antagonist” because contraction of the quadriceps stretches (or antagonizes) most fibers of the ACL. Dr. Michael P. Gillespie