Download
1 / 24
240 likes | 692 Views
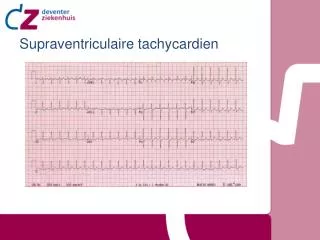
Supraventriculaire tachycardien. Inhoud. Inleiding Atriale tachycardien Sinustachycardie Atriumtachycardie Atriumfibrilleren Atriumflutter Nodale tachycardien AVNRT AVRT/Cirkeltachycardie. Inleiding. Sinus tachycardie. Sinustachycardie. Tachycardie door snel vuren sinusknoop.

E N D
Inhoud • Inleiding • Atriale tachycardien • Sinustachycardie • Atriumtachycardie • Atriumfibrilleren • Atriumflutter • Nodale tachycardien • AVNRT • AVRT/Cirkeltachycardie
Sinustachycardie • Tachycardie door snel vuren sinusknoop. • > 100 / min • Niet medicamenteuze oorzaken: • Inspanning • Pijn • Hypoxie of hypercapnie • Acidose • Koorts of sepsis • Longembolie • Hyperthyreoidie • Medicamenteuze oorzaken: • Beta-agonisten : Adrenaline, isoprenaline, salbutamol, dobutamine • Sympathomimetica: Amphetamines, cocaine, methylphenidate • Antimuscarine: Antihistaminica, TCAs, carbamazepine, atropine • Overige: caffeine, theophylline, marijuana
Sinustachycardie op het ECG • P-top verdwijnt of fuseert deels met de voorgaande T-top • ‘Camel hump’
Atriale tachycardie • Meestal enkelvoudige focus, meerdere ook mogelijk • Mechanisme: re-entry, triggered activity of increased automaticity • Oorzaken oa: Digoxine intoxicatie, atriale leasie, overmatige catecholamines, congenitale afwijkingen, idiopatisch • Paroximaal of persisterend • Zelden persisterend, kan resulteren in tachycardie induces cardiomyopathy
Atriale tachycardie op het ECG • Atriale frequentie van > 100/min • P-top morfologie is abnormaal • De as van de P-top is abnormaal • Minimaal 3 identieke ectopischeP-toppen • QRS-complex normaal • De baseline is iso-electrisch • Er kan een fysiologisch AV-block zijn.
Atriumfibrilleren • Uitlokkende factoren (onder andere): • Hypertensie • Kleplijden • Infectie • Electrolytstoornissen • Hyperthyreoidie • Medicatie ( bijv. Sympatomimetica) • Longembolie
Atriumfibrilleren op het ECG Irregulair ritme Geen P-toppen Géén iso electrische baseline
Atriumflutter • Macro re-entry circuit in rechter atrium • Atriale frequentie 200-400/min, meestal 300/min • Fysiologisch AV-block niet alle prikkels worden voortgeleid • Meest voorkomend is 2:1 geleiding, Ventrikelfrequentie ~ 150/min
Atriumflutter op het ECG • Regelmatig ritme ~150/min in combinatie met AV-block • Zaagtand patroon, meest duidelijk in II, III, aVF en V1. • Frequentie kan irregulair zijn door wisselend AV-block • Geen iso-electrische baseline.
AV-nodale re-entry tachycardie (AVNRT) • Regulaire tachycardie ~140-280/min • Komt meer voor bij vrouwen • Ook bij jonge gezonde patienten
AV-nodale re-entry tachycardie (AVNRT) • Langzamebundel (Alfa): Korterefractaireperiode • Snellebundel (Beta): Langzamerefractaireperiode • Uitlokking door een PAC
AV-nodale re-entry tachycardie (AVNRT) op het ECG • Regulairetachycardiezonder P-toppenvoor het QRS-complex • P-toppen die in of net na het QRS-complex vallen • R’ of S-golf
Atrioventriculaire re-entry tachycardie (AVRT) • Cirkeltachycardie • Via accesoire bundel • Orthodroom of antidroom • Pre-excitatie • Wolff-Parkinson-White • Bundel van Kent
Calciuminstroom-blokkerende middelen • De zijn op grond van hun chemische structuur te verdelen in: • fenylalkylaminen (verapamil); • benzothiazepinen (diltiazem); • dihydropyridineverbindingen ofwel de nifedipinegroep (amlodipine, barnidipine, felodipine, isradipine, lacidipine, lercanidipine, nicardipine, nifedipine, nimodipine, nitrendipine). • Calciumantagonisten blokkeren de instroom via de langzame calciumkanalen en verminderen de binnenkomst van extracellulair calcium, waardoor ze de prikkelgeleiding en contractie van hartspiervezels en gladde spieren in de vaatwand kunnen doen afnemen. Ze hebben geen invloed op de serumcalciumconcentratie. Deze werking resulteert in de volgende effecten: • vertraging in de prikkelgeleiding in SA- en AV-knoop; • vasodilatatie (coronair en systemisch), waardoor o.a. de bloeddruk kan dalen; • en bij sommige een negatief-inotroop effect.
Atrioventriculaire re-entry tachycardie (AVRT) Pre-excitatie in WPW via bundel van Kent
Atrioventriculaire re-entry tachycardie (AVRT)op ECG • PR interval < 120 ms • Delta golf • QRS duurverlengd • T-top afwijkingen