Download
1 / 14
160 likes | 184 Views
This study analyzes the interpatient variability and response to Clopidogrel and Prasugrel in platelet inhibition. It delves into their efficacy, safety, and outcomes in cardiovascular events. Adapted from clinical trials, this study presents key data to aid in treatment decisions.

E N D
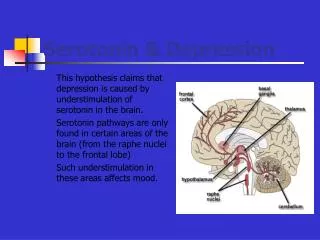
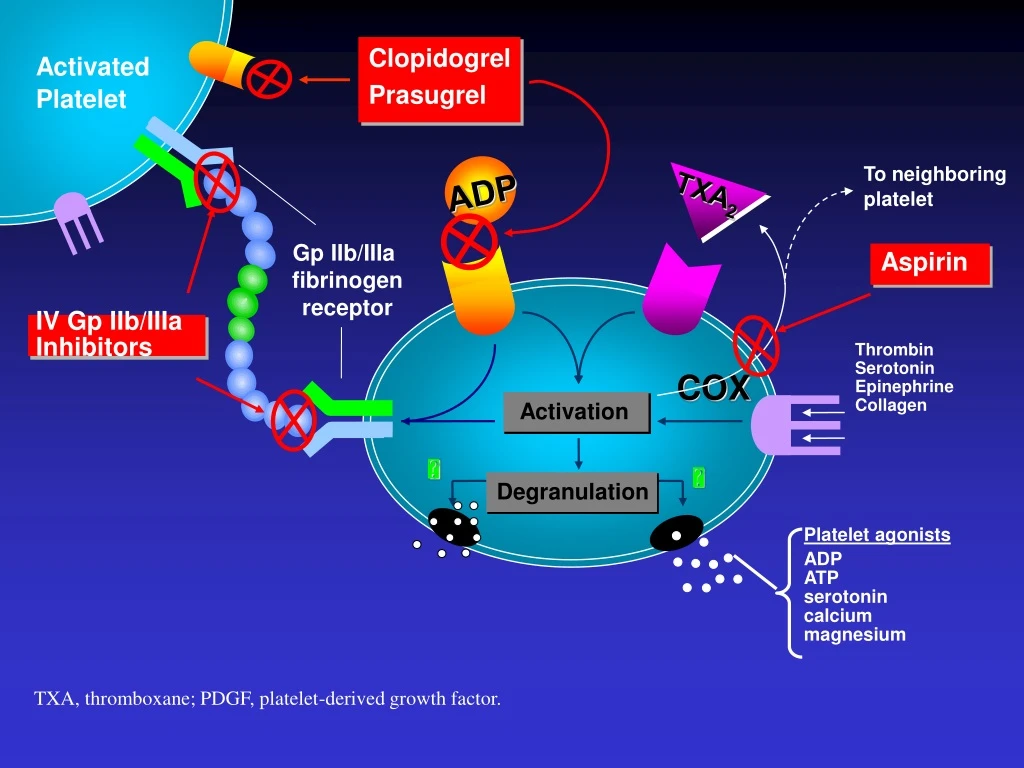
IV Gp IIb/IIIa Inhibitors Aspirin TXA2 ADP Activated Platelet Clopidogrel Prasugrel To neighboring platelet Gp IIb/IIIa fibrinogen receptor Thrombin Serotonin Epinephrine Collagen COX Activation Degranulation Platelet agonists ADP ATP serotonin calcium magnesium TXA, thromboxane; PDGF, platelet-derived growth factor.
Healthy VolunteerCrossover Study 100 N=66 80 InterpatientVariability 60 IPA at 24 hours (%) 40 InterpatientVariability 20 Clopidogrel Responder 0 Clopidogrel Non-responder -20 Response to Prasugrel 60 mg Response to Clopidogrel 300 mg From Brandt JT AHJ 153: 66e9-66e16,2007
TRITON: Primary EndpointCV Death,MI,Stroke 15 Clopidogrel 12.1(781) 9.9 (643) 10 Primary Endpoint (%) Prasugrel HR 0.81(0.73-0.90)P=0.0004 HR 0.80P=0.0003 HR 0.77P=0.0001 5 NNT= 46 LTFU = 14 (0.1%) ITT= 13,608 0 0 30 60 90 180 270 360 450 Days
TRITON TIMI 8 Bilancio efficacia/sicurezza in pz<75 Yrs, ≥60 kg, e senza pregresso TIA/Stroke 1 6 CV Death / NF MI / NF Stroke 1 4 NNT37 Clopidogrel 11% 1 2 Hazard Ratio, 0.75 (95% CI, 0.66-0.84) P<0.001 1 0 Endpoint (%) 8 Prasugrel 8.4% 6 Non-CABG TIMI Major Bleeding Hazard Ratio, 1.240 (95% CI, 0.91-1.69) P=0.17 NNH222 4 Prasugrel 1.95% 2 Clopidogrel 1.50% 0 0 30 90 180 270 360 450 Days Adapted from Wiviott SD et al NEJM 357: 2001, 2007 Presented at TCT 2009, San Francisco, CA
Prasugrel: a chi darlo? • Rischio emorragico • Comorbidita’ • STEMI versus NSTEMI • Eventi ricorrenti • Trombosi di stent
TRITON: sottogruppo dei pazienti con STEMI Endpoint di sicurezza Endpoint di efficacia Wiviott SD et al . N Engl J Med 2007
Randomized Subjects (13608) Any PCI No PCI (195) (13413) Any Stent(12844) No Stent (569) P=6422, C=6422 Mixed BMS Only (6461) DES Only (5743) BMS/DES P=3237, C=3224 P=2865, C=2878 (640) Other or PES Only (2766) SES Only (2454) Mixed DES P=1404, C=1362 P=1210, C=1244 (523) Distribution of Subjects in the TRITON – TIMI 38 Trial Wiviott SD et al. Lancet 2008;371(9621):1353-1363 BMS = bare metal stent; C = clopidogrel; DES = drug-eluting stent; PES = paclitaxel eluting stent; PCI = percutaneous coronary intervention; P = prasugrel; SES = Sirolimus eluting stent
Clinical Events by Stent Type(Any Stent) Pras (%) Clop (%) 10 12 Primary Endpoint (CV death/non-fatal MI/non-fatal stroke CV death/non-fatal MI/UTVR 10 12 CV death/non-fatal MI 9 11 CV death 2 2 MI 7 10 UTVR 2 4 Revascularization 4 6 TIMI major bleeding 2 2 Death/non-fatal MI/non-fatal stroke/non-fatal TIMI major bleed 12 14 0.5 0.6 0.7 0.8 0.9 2.0 Hazard Ratio Prasugrel better Clopidogrel better Wiviott SD et al. Lancet 2008;371(9621):1353-1363
ARC Definite or Probable Stent Thrombosis (day 0 to day 450) 2.5 Clopidogrel 2.35 HR 0.48 (0.36-0.64); P<0.0001 2.0 1.5 % of Subjects 1.13 1.0 Prasugrel 0.5 1 year: 1.06 vs. 2.15% HR 0.48 (0.36-0.65); P<0.0001 0.0 0 50 100 150 200 250 300 350 400 450 Days Wiviott SD et al. Lancet 2008;371(9621):1353-1363 ARC = Academic Research Consortium
ARC Definite or Probable Early Stent Thrombosis (0–30 days) in Patients Receiving DES 2.5 HR 0.29 (0.15-0.56); P=0.0001 2.0 Clopidogrel 1.5 % of Subjects 1.44 1.0 Prasugrel 0.5 0.42 0.0 0 5 10 15 20 25 30 Days Wiviott SD et al. Lancet 2008;371(9621):1353-1363 ARC = Academic Research Consortium; DES = drug-eluting stent
ARC Definite or Probable Late Stent Thrombosis* in Patients Receiving DES 2.5 2.0 HR 0.46 (0.22-0.97); P=0.04 1.5 % of Subjects 0.91 1.0 Clopidogrel 0.5 Prasugrel 0.42 0.0 30 90 150 210 270 330 390 450 Days *Using landmark analysis for all patients, with events occurring from 0–30 days censored from the analysis Wiviott SD et al. Lancet 2008;371(9621):1353-1363 ARC = Academic Research Consortium; DES = drug-eluting stent