Download
1 / 24
240 likes | 555 Views
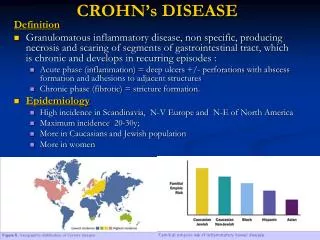
Crohn,s disease. DEFINITION. IBD> RESULT FROM AN ABNORMAL LOCAL IMMUNE RESPONSE AGAINST THE NORMAL FLORA OF THE GUT. CROHN’S DISEASE is a systemic non- caseating granulomatous inflammatory disease with predominant GI-involvement.

E N D
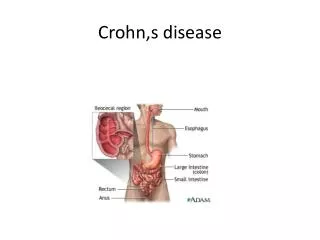
DEFINITION. • IBD> RESULT FROM AN ABNORMAL LOCAL IMMUNE RESPONSE AGAINST THE NORMAL FLORA OF THE GUT. CROHN’S DISEASE is a systemic non-caseatinggranulomatous inflammatory disease with predominant GI-involvement. >may affect any part of GIT from lips to anal margin but most commonly affects terminal ileum.
AETIOLOGY • 1- idiopathic • 2-some proposed risk factors are • >DNA of M.PARATUBERCULOSIS has been found in the intestine of 60%pts but of no value. • >focal ischemia • >dietary habit--------in conclusive • >smoking • >genetic factors
PATHOGENESIS • Pathogenesis of IBD involves 3 components. • 1)Genetic Predisposition, • HLA DR7 and DQ4 alleles. • NON-HLA genes NOD2(CARD15). • (NOD2 protein is an intracellular receptor for muramyldipeptide, a component of cell wall of many bacteria.Mutation in this gene leads to defective host response to bacteria and thus allowing chroinc inflammation.)
2)Immunological Factors, • Primary damaging agents appear to b CD4+ cells. • produce IL-17 and TNF which result in chronic immunological response and tissue inflammation. 3)Microbial Factors, Organisms just provide the antigenic trigger to already dysregulated immune system.
PATHOLOGY • Fibrotic thickening of intestinal wall with a narrow lumen. • Creeping fat • Stricture with deep mucosal ulcers(snake-like pattern) • Oedema in the mucosa b/w ulcers (cobblestone appearance) • Skip lesions
CLINICAL FEATURES A)ACUTE CD: -mimic the C/F of appendicitis with severe diarrhoea -local or diffuse peritonitis -acute colitis with or without toxic megacolon B)CHRONIC CD: 1-1st stage– mild diarrhoea, colicky pain, anemia, mass in the RIF9tender,firm and non mobile) and perianal fissure or abscess.
2-2ND stage---acute or chronic I.O due to fibrosing lead to narrowing. • 3-3RD Stage---adhesions, fissures,intra abdominal abscesses and fistlae formation. • >enteroenteric fistula. • >enterovesical fistula-----recurrent UTI and pneumaturia. • >enterocutaneous fistula.
C)ANAL DISEASE, -bluish perianal skin -painless superficial ulcers with undermined edges -deep ulcers in upper anal canal ass/with perianal abscess and fistula. -sepsis -thick,nodular and irregular rectal mucosa if involved---------rare
D)EXTRAINTESTINAL MENIFESTATIONS: • Skin----erythemanodosum • Eye----iritis, uveitis • Joints---arthritis, • Sclerosingcholangitis • Nephrotic syndrome • Pancreatitis • amyloidosis
INVESTIGATIONS • 1-Laboratory; • -CBC------anemia ,FALL IN ALBUMIN.MAGNESIUM,Zn • -CRP • 2-ENDOSCOPY; • Sigmoidoscopy----ulceration in anal canal • Aphthoid like ulcers surrounded by a rim of erythematous mucosa • strictures
3)Imaging; a)Barium enema--- >narrowed and irregular involved area >string sign of kantor b)sinograms----enterocutaneous fistula c)CT scan-----fistula, intra-abd. Abscesses d)MRI
MANAGEMENT • LIFESTYLE MODIFICATION… • Stop smoking • Eating small meal frequently instead of big meal • Low fiber diet when fiberious food cause symptoms
MANAGEMENT a)MEDICAL THERAPY. >STEROIDS-------------mainstay of therapy >antibiotics---------meteronidazole especially in perianaldisese >immunomodulatory agents----azathioprin, ciclosporin >monoclonal antibody----infliximab >nutritional support----anemia,electrolytes, vitamins etc.
MANAGEMENT b)SURGICAL THERAPY. >Indications -failure of medical treatment -recurrent I.O -fistula formation -bleeding -perforation -malignant changes Perianal disease
MANAGEMENT *PROCEDURES* 1-ileocaecal resection 2-Segmental resection 3-colectomy and ileorectalanastomosis----wide spread colonic disease wd rectal sparing. 4-emegency colectomy 5-laparoscopic surgery 6-temporary loop ileostomy
MANAGEMENT-------- 7-proctocolectomy 8-strictureplasty -----------------------------------
PROGNOSIS • Small bowel and colorectal carcinoma