Download
1 / 12
120 likes | 244 Views
Clinical Programmes Gloucestershire. Commissioning for outcomes Justine Rawlings Associate Director Clinical Programmes. Introduction. Clinical programmes: Based on 23 programme budgeting categories Benchmarked spend and outcomes for these areas

E N D
Clinical Programmes Gloucestershire Commissioning for outcomes Justine Rawlings Associate Director Clinical Programmes
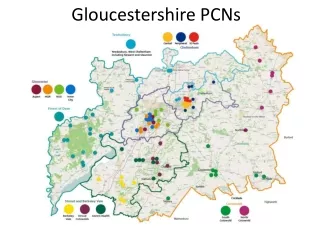
Introduction • Clinical programmes: • Based on 23 programme budgeting categories • Benchmarked spend and outcomes for these areas • Identify priority programme areas for which we are an outlier • Priority programmes for our focus in next 2 years
MSK outcomes • The national SPOT tool suggested the following benchmarked outcomes: • MSK: Initially higher spend average outcome. Now higher spend is decreasing and outcome still average. Note: spend/head has stayed roughly the same as cluster average • Trauma: initially higher spend and lower outcome. Spend has decreased over the years, but outcomes still below average • (Outcomes used by SPOT tool MSK: hip replacement and knee replacement; EQ-5D Health gain 2010/11; Oxford hip score health gain 2010/11 (HES online); Trauma: Mortality from accidents DSR; Mortality from accidental falls DSR, Mortality from fractured NOF, Mortality from skull fracture and intercranial injury, Mortality from land transport accidents)
2015/16: Focus to reduce to quartile benchmarked position Reconstruction – this in large part relates to reconstruction following initial joint replacement surgery and so cannot be delivered as a saving until the initial surgery rate is reduced. NB Reconstruction will be 10-15 years after the initial surgery
Service context • Some evidence of demand management in areas where there was a physiotherapy interface service • Some evidence that patients being referred that do not require surgery • Variation in provision/use of of interface and core physiotherapy service and conservative management options e.g. weight loss programmes
CPG set up • Clinical and managerial representation commissioners and providers • JD for consultant and GP lead including commitment to take back and consult within organisation and provide overall view • Layworker rep and healthwatch rep • Commitment to doing what makes clinical sense for the patient
Developing criteria and guidelines • Detailed guidelines developed for all major joints • Included advice and best practice for GP, physio, interface and surgical IFR criteria • BUT • Thresholds ambiguous if you wanted to use it to manage flow/demand manage
Strengthening thresholds • Clinical workshop review of guidelines and simplifying: • what needs to be done prior to surgical referral • E.g. conservative management and timescale • Weight loss • Patient wants surgery *(shared decision making) • Clear IFR policies for surgical intervention that will be auditable and audited
Outcomes • National outcome measures not comprehensive • We need measures for whole pathway not single providers • Agreed principles and framework aligned to National Outcomes Framework • In first year increased range of PROMs and use EQ5DL
Principles Suggested principles for agreed outcome measures are: • The number of measures should be kept to those that are meaningful, measurable and likely to be used • Measures are for the whole MSK population and are NOT the same as provider based performance measures i.e. one patient may have multiple interventions from multiple providers which influence the outcome • The measures should be applied to conditions that can demonstrate: • Amenability to intervention • Sensitivity to intervention • The scope of outcomes measured should include both measures that are patient reported and service level outcome measures (i.e. no patient input to measure required.) • Process measures can be used as proxies if useful where no suitable outcome measure exists (particularly in order to capture intermediate measures where outcomes are longer term) • Measures, including mode of delivery should be consistent across services and providers • Measures should be appropriate to an intervention and should include measures for interventions dealing with prevention, episodic care and interventions for chronic conditions. • Measures should take account of the whole pathway, ideally across all interventions including where a patient has declined or not been accepted for an intervention. (e.g. where shared decision-making has been part of the process)
Further work One system one budget • Care pathways programme • Single approach to service development In year programmes to support • Advice and guidance • Peer review