Download

1 / 77
810 likes | 1.79k Views
Neuropsychological Perspectives on Long-Term Memory Problems in Children and Adolescents. Milton J. Dehn, Ed.D., NCSP Schoolhouse Ed. Services mdehn2@msn.com. Long-Term Memory (LTM) Topics. Systems and processes Brain structure Development At-risk populations Assessment Instruction

E N D
Neuropsychological Perspectives on Long-Term Memory Problems in Children and Adolescents Milton J. Dehn, Ed.D., NCSP Schoolhouse Ed. Services mdehn2@msn.com
Long-Term Memory (LTM) Topics • Systems and processes • Brain structure • Development • At-risk populations • Assessment • Instruction • Intervention
Why Is This Important? • A frequent underlying impairment • Advances in neuroscience • Under-identified in children & adolescents • A growing problem, e.g, juvenile diabetes • Evidence-based interventions available • Needs to be included in more evaluations
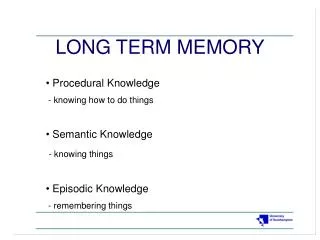
LTM Memory Systems • Explicit/declarative • Episodic • Semantic • Implicit/nondeclarative • Priming • Procedural Learning • Classical conditioning
Explicit vs Implicit • ExplicitImplicit • Conscious Unconscious • Knowledge Skills • Flexible expression Rigid expression • Hippocampus-dependent Non-hippocampus • Recollection expressed Performance expresses • Cognitive only Non-cognitive also • Effortful retrieval also Automatic retrieval only • Develops until adulthood Developed by age three • Vulnerable to injury Resistant to injury
Episodic vs Semantic • EpisodicSemantic • Memory for events Memory for facts • Remembering Knowing • Context dependent Context free • Subjective focus Objective focus • Vulnerable to pathology Resistant to pathology • Develops later Develops first • Known source Unknown source • Mostly visuospatial Mostly verbal • Unintentional encoding More intentional • Chronological Categorical • Organized spatiotemporally Organized by meaning • Subject to rapid forgetting Less rapid forgetting
Episodic-Semantic Interactions • School learning is initially episodic but eventually semantic • Episodic helps build the semantic • Semantic provides the schemas and scripts for the episodic • Memory tests are episodic • Must use IQ subtests for semantic
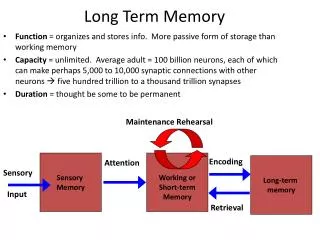
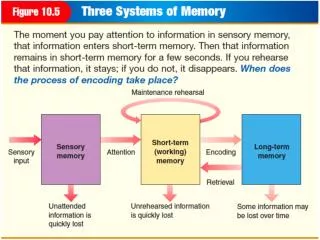
Flow of Information • Environment • Sensory Memory • STM • WM • LTM • Expression • Flow Link • Systems interaction link
STM vs LTM • STMLTM • Very limited capacity Extensive capacity • Retention for seconds Retention for minutes to years • Conscious access to all content Limited conscious access • Only two types Multiple types • Depends on attention Less dependent on attention • Immediate retrieval only Retrieval can be extended • Forgetting is immediate Forgetting is gradual • Amenable to simple strategies Amenable to elaborate strats. • Easy to assess Difficult to assess • Less susceptible to brain injury Very susceptible to brain injury The chimpanzee?
LTM Processes • Encoding • Consolidation • Storage • Retrieval • Forgetting
Encoding • Requires attention • Associated with learning • All other memory depends on • Enhanced by strategies • Hippocampus dependent
Learning • Mainly refers to initial learning, encoding, and short-term recall • Learning curve---improves rapidly then plateaus • What is difficult to learn is difficult to remember and vice versa • Can be separated from memory---same degree of learning but different retention
Forgetting • Fast at first, then slows down • 50% forgotten within 24 hours • Some retain well within 30 minutes or 1st day but then have very poor retention afterwards • Is it lost, or not retrievable at moment • Interference: proactive and retroactive
Consolidation • Often ignored • Evidence from TBI and amnesia • Takes time • Unconscious mostly • Movement from medial temporal lobe/hippocampus to cortical areas • Episodic to semantic • Much of it occurs during sleep
Storage • Memory traces---changes in strength of synapses • In networks of interconnected neurons • Depends on the pathways between neuronal networks • Memories end up being stored in same areas that sensed, perceived, and processed incoming information
Retrieval • Mostly automatic • WM involved in effortful retrieval • Hippocampus “pulls together” information • Reasoning involved in reconstruction • If can recognize but can’t recall problem is with retrieval, not storage
LTM and the Brain Lobes • Temporal lobes---most memory functions • Frontal lobes---memory strategies • Parietal---storage; auditory and spatial • Occipital---storage; visuospatial
The Hippocampus • Horseshoe shape in temporal lobe • Sensitive to injury, glucose, cortisol • Necessary for STM-LTM transfer • Consolidates and re-integrates • May hold some episodic long-term • Explicit memory only
Other Brain Structures • Amygdala---emotional content; more implicit than explicit memory • Thalamus---memory relay station
Memory Development • Memory structures fully developed by age 6 except those related to exec. functions • Consistent improvements in retention • Due to expanded background knowledge • Due to growth of effective strategies • Retained episodic memories by age 3 • Semantic before episodic (infantile amnesia) • Implicit before explicit
Metamemory • More than self-awareness • Knowing what you know • Judgments of learning • Understanding memory functions • Monitoring and regulating • Strategy knowledge and monitoring • Conditional knowledge • Absolutely essential intervention piece
Judgments of Learning • More accurate with age • Overly optimistic • Influences what is studied and for how long but average student still does not study difficult material long enough • Fooled by STM retrieval and not taking forgetting into account
Memory Strategies • Simple strategy use by age 3 • After age 6, account for LTM improvement • Strategy use and recall (r = .81) • From simple to complex to integrated • Use depends on metamemory (r = .41) and knowledge of efficacy • Development spurred by academic requirements
Disorders and Impairments • Amnesia: Retrograde and anterograde • Impairments: • Verbal Visuospatial • Episodic Semantic • Encoding Consolidation • Storage Retrieval • Metamemory Strategic
At-Risk Conditions, Disorders • Risk created by damage to hippocampus • Sometimes, damage to prefrontal cortex • Some present at birth or early infancy; others acquire later • Some temporary with recovery, some stable, some progressively worse • Limitation: More adult than child research for most conditions
TBI • .25% of youth acquire a TBI each year • Severe TBI: 36 – 53% have ongoing impairments in LTM • Implicit more resistant to injury • More verbal problems than visuospatial • Most mild cases recover within a month • But some can have persistent problems • Most moderate cases within 1-2 years • Metamemory when frontal lobes involved
TBI Example • Fractured skull (parietal area) as infant • Surgery; surgeon predicted no LTM deficit • Normal development at age 3 • Expressive language delays in kindergart. • Spec. Ed. by grade 3 • Memory problems at home evident • Deficits in STM, WM, and LTM • Problems: Encoding, storing, retrieving • Delayed strategy development
Post-Concussion Syndrome • 19% chance school athlete per year • Likely memory problems: few days/weeks • Loss of consciousness increases risk • Possibility of persistent LTM problems should be considered • Athletes will deny so they can play again • Pre-season baseline testing important • Example: Soccer player
Type I Diabetes • Hippocampus sensitive to glucose levels • Growing numbers of diabetic children • Greater risk with earlier onset • Greater risk with poorly controlled insulin • Hypoglycemia damages hippocampus • Memory functions decline over time • Children of diabetic mothers also at risk • Even nondiabetics with poor insulin control
Epilepsy • 10% have significant memory impairment • Depends on type, severity, frequency, and location of seizures • Temporal lobe type most devastating • Especially known for “accelerated forgetting” • Seizures disrupt consolidation
PTSD • Due to abuse, trauma or witnessing violence • More PTSD symptoms, more LTM deficits • Vietnam PTSD; 26% hippocamp reduction • Cortisol damages hippocampus • Temporary elevated cortisol reduces encoding • Chronic stress causes LTM problems
FAS and Alcohol Consumption • FAS children have a smaller hippocampus • Even mild alcohol consumption increases risk for LTM problems, which usually go undetected • Effects are dose-dependent • Difficulty inhibiting interference
Language-Impaired • Adequate phonological STM is essential • Problems with encoding, retrieval, semantic memory • Difficulty with rehearsal strategies • Retention is okay once they have learned material
LD • Also, STM and WM problems • LTM problems usually unidentified • Verbal with reading and writ. lang. • Visuospatial with math • Encoding is primary dysfunction • Slow retrieval frequently a concern
Developmental Amnesia • Recent research on these cases • Often from prenatal, perinatal, neonatal risk-factors • May learn okay despite severe problems with episodic retention and everyday memory problems • Structure and parental monitoring masks their real memory functioning
Other Conditions/Disorders • See handout chart for others along with most likely specific memory impairments • Handout
Assessment Challenges • Time consuming • Cognitive abilities versus strategy usage • Everyday vs formal test activities • Episodic vs semantic • Difficult to isolate memory processes • Tests don’t check long-term forgetting • Poor labeling on standardized measures • Influence of STM, WM, other processes
Assessment Strategies • Generate memory hypotheses based on concerns, observations, existing data • All informal methods important • Select memory types and processes • Select batteries and subtests • Include verbal and visuospatial • Include STM and LTM • Consider everyday memory
History • Development and health are essential • Consider risk factors • Academic markers • Progress worse as memory demands increase • Studies but performs poorly on exams
Observations • Attention • Opportunities to encode • Mnemonic classroom environment • Evidence of strategy use • Retrieval speed and difficulty • Recognition vs retrieval
Interviews • Examinee, parents, teachers • Unrealistic child implicates metamemory • Poor memory for non-academics • Is the info. being encoded adequately • Strategy use • Rate of learning and rate of forgetting
Metamemory Assessment • A standardized measure is lacking • Knowledge of memory functions • Knowledge of LTM strengths/weaknesses • Accuracy of JOL’s • Knowledge of strategies See handout of interview item examples
LTM Test Chart • See handout of instruments and types of memory assessed • Sign up to receive copy via email
Semantic Memory Assessment • Need to use verbal subtests from IQ and other tests • Information, Vocabulary, Similarities, Academic Knowledge • Classroom exam performance • Vocabulary development
WMS-IV • 2009, Pearson; ages 16-90 • Co-normed with WAIS-IV • Fewer subtests/factors than WMS-III • Primarily a measure of declarative episodic memory (novel & contextually bound)
WMS-IV Structure • Immediate and Delayed: 4 subtests each • Auditory and Visual: 4 subtests each • Visual Working Memory • 2 subtests (not part of above factors) • Brief Cognitive Status • 11 subtests (counting delayed versions) • Must compute clinical factors for auditory delayed and visual delayed
Learning Disabled ReadingMath Immediate 98.1 89.1 Delayed 96.6 91.7 Auditory 99.5 92.4 Visual 95.0 91.1 VWM 100.1 89.0
Logical Memory I and II • Narrative memory under free recall • Consists of 2 short stories presented orally • New story for ages 65-90 that has less language demand and is more age approp • Story A is presented twice • Do II 20 – 30 minutes later • Video
Design Memory I and II • Examinee is presented with 4 to 8 designs on a grid, cards with designs and foils to place on grid; scored for correct location and correct design independently, with bonus for both • Scores: Immediate Spatial, Immediate Content, Immediate Total, Same 3 Delayed scores, Delayed Recognition • See DE I See DE IISee DE II Recognition