Download
1 / 21
210 likes | 471 Views
Cryptococcal Meningitis Sam Nightingale

E N D
Cryptococcal Meningitis Sam Nightingale Sam Nightingale is a neurology registrar and MRC clinical research fellow. He is currently working with the Liverpool HIV Pharmacology Group and the Liverpool Brain Infections Group setting up a multicentre UK study to look at the CNS penetration of antiretrovirals. Edited by Prof Tom Solomon and Dr Agam Jung • Cryptococcal • Meningitis • Learning Objectives • Introduction • C.Neoformans • C. Gatti • Clinical Features • Space Occupying Cryptococcus • IRIS • Cryptococcus in other sites • Diagnosis • Extra-neurological • Management • Prognosis • Key Points • Summary • Self assessment This session provides an overview of cryptococcal meningitis in healthy and immunocompromised individuals.
Learning Objectives • By the end of this session you will be able to: • List the similarities and differences between the 2 main species of cryptococcus causing CNS disease in humans • Summarise the presentation and clinical features of cryptococcal disease both within the CNS and systemically • Given a set of laboratory and CSF parameters, correctly differentiate fungal meningitis from other aetiologies • Outline the principles of management of cryptococcal meningitis • Cryptococcal • Meningitis • Learning Objectives • Introduction • C.Neoformans • C. Gatti • Clinical Features • Space Occupying Cryptococcus • IRIS • Cryptococcus in other sites • Diagnosis • Extra-neurological • Management • Prognosis • Key Points • Summary • Self assessment
Introduction • Cryptococcal • Meningitis • Learning Objectives • Introduction • C.Neoformans • C. Gatti • Clinical Features • Space Occupying Cryptococcus • IRIS • Cryptococcus in other sites • Diagnosis • Extra-neurological • Management • Prognosis • Key Points • Summary • Self assessment Cryptococcus neoformans and Cryptococcus gattii are encapsulated yeast, which can be inhaled from the environment. Usually this results in harmless colonisation of the airways. However in some situations, it may lead to disseminated disease including serious and life threatening meningitis. Most infections are associated with immunosuppression and around 80%-90% of all patients with cryptococcosis have advanced HIV infection. Cryptococcosis is an AIDS defining illness. Worldwide up to 15% of those with AIDS will develop cryptococcal meningitis at some time. Incidence varies and in parts of sub-Saharan Africa over 50% of those with HIV are affected. In addition, CNS cryptococcosis is frequently associated with immune reconstitution inflammatory syndrome (IRIS). There are over 50 species of Cryptococcus. However only Cryptococcus neoformans and Cryptococcus gattii are considered pathogens in humans.
Cryptococcus Neoformans This is a ubiquitous fungus found predominantly in aged bird droppings. Clinically evident infection usually only occurs in those with significant defects in cell mediated immunity. By far the most common cause is AIDS. However Cryptococcus neoformans can affect people with reticuloendothelial malignancy, organ transplant recipients, sarcoidosis and those on long term steroids. • Cryptococcal • Meningitis • Learning Objectives • Introduction • C.Neoformans • C. Gatti • Clinical Features • Space Occupying Cryptococcus • IRIS • Cryptococcus in other sites • Diagnosis • Extra-neurological • Management • Prognosis • Key Points • Summary • Self assessment
Cryptococcus Gattii Cryptococcus gattii is not associated with birds but grows in the litter around certain species of eucalyptus tree. It is most common in tropical and subtropical areas. The highest incidence is in Papua New Guinea and Northern Australia, although infections occur in non-tropical areas such as North America and Europe. Patients infected with Cryptococcus gattii are usually immunocompetent. In contrast to Cryptococcus neoformans, Cryptococcus gattii rarely infects immunosuppressed patients and is not associated with HIV infection. Intracerebral mass lesions (Cryptococcomas) are more common with Cryptococcus gattii than in Cryptococcus neoformans, presumably due to their different host immune responses. • Cryptococcal • Meningitis • Learning Objectives • Introduction • C.Neoformans • C. Gatti • Clinical Features • Space Occupying Cryptococcus • IRIS • Cryptococcus in other sites • Diagnosis • Extra-neurological • Management • Prognosis • Key Points • Summary • Self assessment
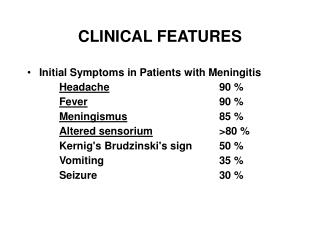
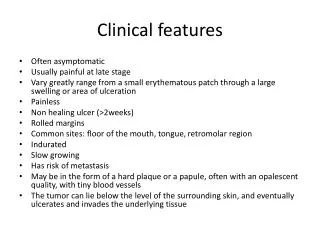
Clinical Features A typical acute presentation is headache and mild fever, often accompanied by nausea and vomiting for a few days. Subacute and chronic presentations can mimic other meningitides, particularly tuberculous meningitis, but with cryptococccal infection, there tends to be a less aggressive meningeal inflammatory response. For example, only one third of patients have classical features of meningism, such as photophobia, neck stiffness or positive Kernig's sign. • Cryptococcal • Meningitis • Learning Objectives • Introduction • C.Neoformans • C. Gatti • Clinical Features • Space Occupying Cryptococcus • IRIS • Cryptococcus in other sites • Diagnosis • Extra-neurological • Management • Prognosis • Key Points • Summary • Self assessment Severely immunocompromised patients may just have nonspecific symptoms at presentation. In some cases the only feature may be confusion, with or without a low-grade fever. Cryptococcal infection prevents the arachnoid granulations from resorbing CSF effectively. As a result almost all have raised intracranial pressure. CSF pressure can become dangerously high causing papilloedema and communicating hydrocephalus.
Space Occupying Lesion Cryptococcomas • Cryptococcal • Meningitis • Learning Objectives • Introduction • C.Neoformans • C. Gatti • Clinical Features • Space Occupying Cryptococcus • IRIS • Cryptococcus in other sites • Diagnosis • Extra-neurological • Management • Prognosis • Key Points • Summary • Self assessment CNS parenchymal invasion leads to abscesses and granuloma in up to 11%. Lesions are round, often multiple and may or may not enhance. The common differentials of CNS space occupying lesions HIV are toxoplasmosis, primary CNS lymphoma or tuberculomas. Clinical presentation depends on the location of the lesions. Focal neurological signs and seizures are common. Lesions can occur throughout the CNS but are more common in the basal ganglia and cerebellum. In addition, invasion of blood vessels can result in cerebral infarction Figure: T2 MRI showing cryptococcomas in the posterior fossa of an HIV positive individual. Image courtesy of Ian Turnbull.
Cryptococcal immune Reconstitution Inflammatory Syndrome (IRIS) • Cryptococcal • Meningitis • Learning Objectives • Introduction • C.Neoformans • C. Gatti • Clinical Features • Space Occupying Cryptococcus • IRIS • Cryptococcus in other sites • Diagnosis • Extra-neurological • Management • Prognosis • Key Points • Summary • Self assessment Immune reconstitution inflammatory syndrome (IRIS) describes a phenomenon where HIV positive patients starting antiretroviral therapy develop atypical manifestations of opportunistic pathogens as CD4 count improves. Cryptococcal IRIS may present as a clinical worsening or new presentation of cryptococcal disease following antiretroviral treatment, particularly if treatment was started at a low CD4 count and immune recovery was rapid. It is thought to be caused by recovery of cryptococcus specific immune responses. Cryptococcal IRIS may present with lymphadenitis, meningitis or pulmonary lesions. Intracerebral mass lesions are more common due to the increased inflammatory response. It tends to occur a few months after starting antiretroviral therapy, but can occur some years later and so is often difficult to diagnose. IRIS does not represent treatment failure or reactivation of infection and therefore does not require antifungal therapy. Treatment is aimed at controlling the inappropriate immune response and systemic corticosteroids are beneficial.
Cryptococcosis in Other Sites • Cryptococcal • Meningitis • Learning Objectives • Introduction • C.Neoformans • C. Gatti • Clinical Features • Space Occupying Cryptococcus • IRIS • Cryptococcus in other sites • Diagnosis • Extra-neurological • Management • Prognosis • Key Points • Summary • Self assessment Cryptococci disseminate widely and may infect any organ, most commonly lymphadenitits, prostatitis and skin or bone lesions. Cutaneous manifestations occur in 10%-15% of cases. Umbilicated papules initially resemble molluscum contagiosum, later becoming confluent and forming larger ulcerated lesions. Pulmonary infection can cause pneumonia, ARDS and cavitating lesions. Although the lung is the presumed site of entry to body, most patients do not have pulmonary symptoms. Bone lesions are usually osteolytic or resemble cold abscesses, sometimes misdiagnosed as tuberculosis. Rarely other organs are involved in causing chorioretinitis, hepatitis and renal abscess. Figure: Field stain showing cryptococci in the lungs.
Diagnosis Imaging Diagnosis must be made without delay as early symptoms can progress rapidly to life threatening illness. There should be a low threshold for lumbar puncture in any HIV positive individual presenting with non-specific symptoms such as mild headache or confusion. • Cryptococcal • Meningitis • Learning Objectives • Introduction • C.Neoformans • C. Gatti • Clinical Features • Space Occupying Cryptococcus • IRIS • Cryptococcus in other sites • Diagnosis • Extra-neurological • Management • Prognosis • Key Points • Summary • Self assessment Brain imaging may reveal communicating hydrocephalus, mass lesions (cryptococcomas) or basal meningeal enhancement. MRI is more sensitive than CT and is particularly useful if there are focal neurological signs. The contrast enhanced CT opposite shows basal menengeal enhancement (1). Hydrocephalus and rained intracranial pressure is demonstrated by the prominent temporal horns (2) and effacement of the sulci (3).
Diagnosis Lumbar Puncture I The most important test for cryptococcosis is lumbar puncture. Even if disease appears to be restricted to organs outside the CNS, a lumbar puncture must be performed to exclude subclinical CNS involvement. In most cases there is a moderate mononuclear cell pleocytosis of around 20 to 200 cells/mm3 although higher counts can be seen. Protein is elevated and CSF/plasma glucose ratio mildly decreased (see table opposite) However the CSF may be normal in up to 25% of cases, particularly in early infection. • Cryptococcal • Meningitis • Learning Objectives • Introduction • C.Neoformans • C. Gatti • Clinical Features • Space Occupying Cryptococcus • IRIS • Cryptococcus in other sites • Diagnosis • Extra-neurological • Management • Prognosis • Key Points • Summary • Self assessment
Diagnosis Lumbar Puncture II Papilloedema is common but not necessarily a contraindication to LP if imaging excludes a space occupying lesion, as it is usually due to communicating hydrocephalus from decreased resorption. As pressure is raised evenly throughout the CSF compartment, there is no increased risk of tentorial or brainstem herniation. In fact, by reducing the CSF pressure, lumbar puncture is essential treatment for raised intracranial pressure in this situation. • Cryptococcal • Meningitis • Learning Objectives • Introduction • C.Neoformans • C. Gatti • Clinical Features • Space Occupying Cryptococcus • IRIS • Cryptococcus in other sites • Diagnosis • Extra-neurological • Management • Prognosis • Key Points • Summary • Self assessment
Diagnosis • Cryptococcal • Meningitis • Learning Objectives • Introduction • C.Neoformans • C. Gatti • Clinical Features • Space Occupying Cryptococcus • IRIS • Cryptococcus in other sites • Diagnosis • Extra-neurological • Management • Prognosis • Key Points • Summary • Self assessment Lumbar Puncture III Definitive diagnosis is established by the identification of fungal hyphae with India ink staining in 60-80%. Repeating lumbar puncture three or more times and centrifuging larger volumes of CSF, increases the diagnostic yield. The detection of cryptococcal antigen (CrAg), a capsular polysaccharide, is more sensitive. It is positive in around 95% of cases and has a high specificity. CSF opening pressure is almost always elevated and may cause ischaemic pressure on the optic nerve threatening sight. Often large volumes of CSF have to be removed to bring the pressure below 20cm H2O. In refractory cases requiring repeated lumbar puncture, a lumbo-peritoneal or ventriculo-peritoneal CSF shunt may be necessary. Acetozolamide which reduces CSF production may help in milder cases. Steroids, which are often helpful in reducing the pressure associated with space occupying lesions, are ineffective in communicating hydrocephalus such as this.
Blood Most HIV-related cryptococcal CNS infections occur at a CD4 count less than 100 cells/ul and are rarely seen at CD4 counts above 200 cells/ul. Full blood count and other routine bloods may be normal even in advanced cryptococcal disease. Fungal blood cultures may be positive indicating disseminated cryptococcaemia. Cryptococcal antigen (CrAg) in the blood at a titre >1:8 is almost as sensitive as CSF. However a falling titre during therapy is not a reliable indicator of when to stop treatment. Blood cultures are also often positive in disseminated disease. • Cryptococcal • Meningitis • Learning Objectives • Introduction • C.Neoformans • C. Gatti • Clinical Features • Space Occupying Cryptococcus • IRIS • Cryptococcus in other sites • Diagnosis • Extra-neurological • Management • Prognosis • Key Points • Summary • Self assessment
Extraneurological • Cryptococcal • Meningitis • Learning Objectives • Introduction • C.Neoformans • C. Gatti • Clinical Features • Space Occupying Cryptococcus • IRIS • Cryptococcus in other sites • Diagnosis • Extra-neurological • Management • Prognosis • Key Points • Summary • Self assessment Extraneurological features may be present in up to 20%. A chest xray may reveal diffuse pulmonary infiltrates, lobar consolidation or cavitating lesions, which may resemble tuberculosis. High resolution CT scan is more sensitive than chest xray if pulmonary involvement is suspected. Bronchoalveolarlavage can identify the causative organism. Cutaneous lesions should be biopsied and evaluated with fungal stains and cultures. Urine should also be cultured even if renal or urinary tract disease is not clinically evident.
Management • Cryptococcal • Meningitis • Learning Objectives • Introduction • C.Neoformans • C. Gatti • Clinical Features • Space Occupying Cryptococcus • IRIS • Cryptococcus in other sites • Diagnosis • Extra-neurological • Management • Prognosis • Key Points • Summary • Self assessment Before treatment was available, cryptococcal meningitis was invariably fatal. With effective treatment the mortality rate remains up to 25%. Treatment is lengthy, complicated and potentially toxic and should initially be managed on an inpatient basis. Standard treatment is with intravenousamphotericin B with oralflucytosine for 2 weeks followed by fluconazole for 8-10 weeks. Fluconazolecan can also be used at induction as a less toxic alternative to amphotericin B, particularly in those with renal impairment. Itraconazole has been shown to be less effective
Management II • Cryptococcal • Meningitis • Learning Objectives • Introduction • C.Neoformans • C. Gatti • Clinical Features • Space Occupying Cryptococcus • IRIS • Cryptococcus in other sites • Diagnosis • Extra-neurological • Management • Prognosis • Key Points • Summary • Self assessment Treatment should be considered successful when CSF culture and constituents have returned to normal, although protein can remain elevated for some time longer. Treatment is curative in immunocompetant individuals. However, in HIV prolonged suppressive treatment is required with oral fluconazole at a lower dose until CD4 count is greater than 200 cells/ul for more than 6 months and serum cryptococcal antigen is negative. Antiretroviral therapy should be continued. When initiating antiretroviral therapy in those with cryptococcal meningitis, prior antifungal treatment may reduce the risk of immune reconstitution inflammatory syndrome (IRIS). Primary prophylaxis or avoidance of exposure has not been shown to be of benefit, even in endemic areas. Cryptococcomas Treatment is the same as for cryptococcal meningitis. Early in therapy new lesions may arise and existing lesions enlarge as a result of the inflammatory response associated with treatment. This does not necessarily represent failure of therapy and lesions tend to shrink over time if treatment is continued.
Prognosis A number of adverse prognostic markers have been identified including abnormal mental status, CSF opening pressure >25 cm H20, CSF cryptococcal antigen titre>1:1024, CSF white cell count >20 cells/ml and culture of cryptococcus outside the CSF. • Cryptococcal • Meningitis • Learning Objectives • Introduction • C.Neoformans • C. Gatti • Clinical Features • Space Occupying Cryptococcus • IRIS • Cryptococcus in other sites • Diagnosis • Extra-neurological • Management • Prognosis • Key Points • Summary • Self assessment Without treatment cryptococcal meningitis is invariably fatal. Despite effective treatment the mortality rate remains up to 25%. Of those who survive, 40% have significant neurological deficits, including loss of vision, decreased cognitive function, and cranial nerve palsies. Hydrocephalus can occur as a late complication. Relapse can occur in up to 25%. Cure may not be possible and in some patients life-long suppressive anti-fungal therapy may be required. Figure: CT scan showing gross obstructive hydrocephalus this can occur as an early or late complication of cryptococcal meningitis
Session Key Points • Cryptococcal • Meningitis • Learning Objectives • Introduction • C.Neoformans • C. Gatti • Clinical Features • Space Occupying Cryptococcus • IRIS • Cryptococcus in other sites • Diagnosis • Extra-neurological • Management • Prognosis • Key Points • Summary • Self assessment • Cryptococcal meningitis can be caused by C. neoformans or C. gattii. C. neoformans affects those with advanced immunosupression, however C. gattii can affect the immunocompetent • Cryptococcal meningitis typically presents with headache, confusion +/- fever. Meningeal irritation is not a prominent feature. Onset may be over weeks. Symptoms are variable and can be mild • Cryptococcus can present as part of an immune reconstitution inflammatory syndrome (IRIS) • Crytptococcal meningitis can be associated with mass lesions (cryptococcomas) • The affect of cryptococcus on CSF resorbtion often causes raised intracranial pressure and papilloedema. However lumbar puncture is not contraindicated as this is a communicating hydrocephalus. • Antifungal treatment is lengthy. In HIV positive patients, suppressive treatment should be continued until immune function has been restored
Summary • Cryptococcal • Meningitis • Learning Objectives • Introduction • C.Neoformans • C. Gatti • Clinical Features • Space Occupying Cryptococcus • IRIS • Cryptococcus in other sites • Diagnosis • Extra-neurological • Management • Prognosis • Key Points • Summary • Self assessment • Having completed this session you will now be able to: • List the similarities and differences between the 2 main species of cryptococcus causing CNS disease in humans • Summarise the presentation and clinical features of cryptococcal disease both within the CNS and systemically • Given a set of laboratory and CSF parameters, correctly differentiate fungal meningitis from other aetiologies • Outline the principles of management of cryptococcal meningitis • References/ further reading • Clin Infect Dis. 2000 Apr;30(4):710-8. Epub 2000 Apr 20.Practice guidelines for the management of cryptococcal disease. Infectious Diseases Society of America. Saag MS et al. • Kaplan JE, Masur H, Holmes KK. Guidelines for preventing opportunistic infections among HIV-infected persons--2002. Recommendations of the U.S. Public Health Service and the Infectious Diseases Society of America. MMWR Recomm Rep. Jun 14 2002;51:1-52. • J Infect. 2005 Dec;51(5):e289-97. Cryptococcal immune reconstitution inflammatory syndrome: report of four cases in three patients and review of the literature.Skiest DJ, Hester LJ, Hardy RD. • The Lancet Infectious Diseases, Volume 10, Issue 11, Pages 791 - 802, November 2010 Cryptococcal immune reconstitution inflammatory syndrome in HIV-1-infected individuals: proposed clinical case definitions Lewis J Haddow PhD ab, Prof Robert Colebunders PhD cd, et al on behalf of the International Network for the Study of HIV-associated IRIS (INSHI).
Question 1 • Cryptococcal • Meningitis • Learning Objectives • Introduction • C.Neoformans • C. Gatti • Clinical Features • Space Occupying Cryptococcus • IRIS • Cryptococcus in other sites • Diagnosis • Extra-neurological • Management • Prognosis • Key Points • Summary • Self assessment Select the single best answer from the options given. Click on the answer to see if it is correct and read an explanation. Bacterial meningitis Cryptococcus neoformans meningitis Cryptococcus gattii meningitis Tuberculosis meningitis Viral meningitis A 35-year-old HIV positive lady with a 3 week history of fever and headache. CD4 count 350 cells/ul. CSF: WCC 200 mm3 (100% lymphocytes). Protein 2g, serum:CSF glucose 25%. Select one answer from the list below.