Chest Xrays
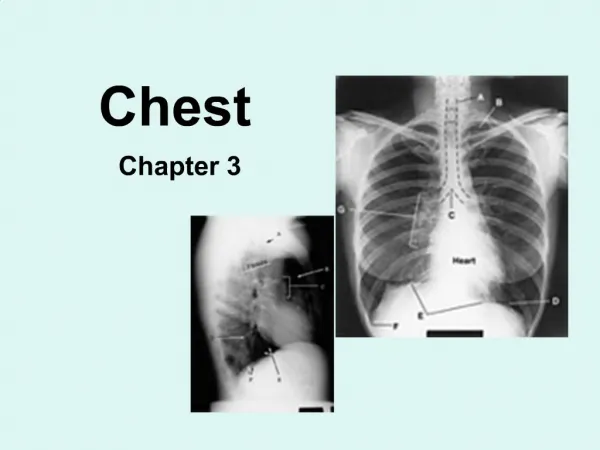
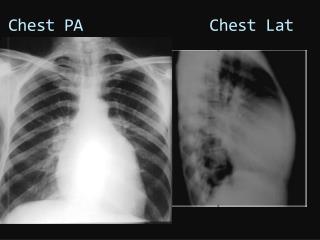
Chest Xrays. Intro. This is a chest radiograph of Mr X who presented with SOB and weight loss This is an AP/PA chest radiograph… The radiograph is adequate Penetrance is… (vertebrae) Rotation adequate (distance between two clavicles) Exposure adequate (can see all of patient!).

Chest Xrays
E N D
Presentation Transcript
Intro • This is a chest radiograph of Mr X who presented with SOB and weight loss • This is an AP/PA chest radiograph… • The radiograph is adequate • Penetrance is… (vertebrae) • Rotation adequate (distance between two clavicles) • Exposure adequate (can see all of patient!)
The most obvious abnormality is… • Consolidation, opacity, loss of lung fields, meniscal sign…etc in the ……
A - airway • Trachea central?
B - Breathing • Lung fields visible? • Prominent hila? • Lymphoma, sarcoidosis, tb, malignant lymphodenopathy • Lung fields not visible? • Pneumothorax (always – tracheal deviation) Rx attempt aspiration if fails chest drain • Primary causes: CT disorders e.g. Marfan’s, Ehler’sDanlos • Secondary causes: trauma, tumour, infection • Tension pneumothorax (always + tracheal deviation) • Consolidation • Upper lobe pneumonia is tb or carcinoma (usually small cell) until proven otherwise • Mass (tumour, hamartoma, tb abscess, aspergillus)
C - Circulation • Cardiac silhouette visible? • Cardiomegaly if PA? • Check behind heart for tumours • Cardiophrenic angles?
D - Diaphragm • Costophrenic angles? • Meniscal sign = effusion • Unilateral effusion is usually exudative i.e. Light’s criteria protein >30g causes incl trauma, tumour, infection • Bilateral effusion usually transudative i.e. Light’s criteria protein <30g, causes are heart failure and hypoalbuminaemia (due to malnutrition, liver failure, nephrotic syndrome) • Pneumoperitoneum
E – everything else • No obvious bony abnormalities or sclerotic lesions
In summary… • This is a 65yo man who presented with SOB and weight loss. The most obvious abnormality is complete opacity of the right lower zone with obliteration of the costophrenic and cardiophrenic angles and meniscal sign consistent with a diagnosis of pleural effusion.
Left lower lobe pneumonias cause loss of L hemidiaphragm and L heart border Right lower lobe pneumonias cause loss of R hemidiaphragm…. Right MIDDLE lobe causes loss of L heart border Easiest to refer to “zones”!