Download
1 / 31

E N D
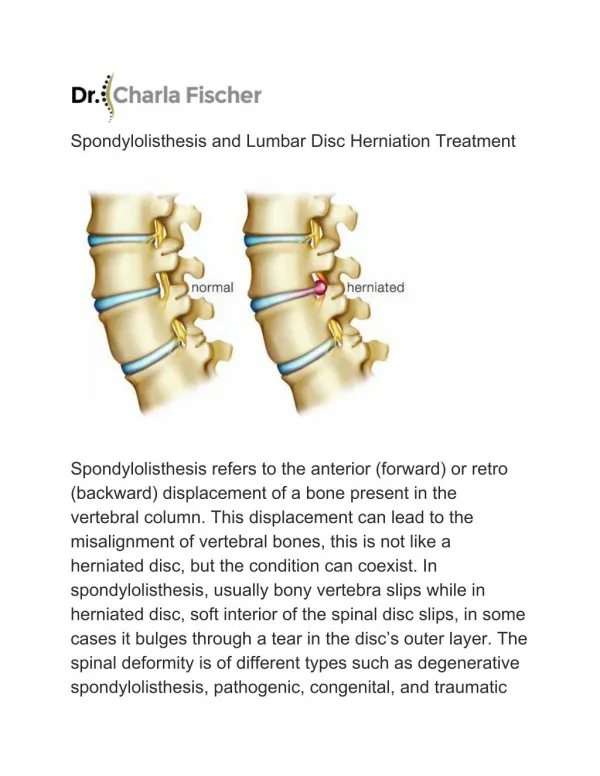
Spondylolisthesis Definition The term "Spondylolisthesis" refers to a condition where one of the vertebrae (usually L5) becomes misaligned anteriorly (slips forward) in relation to the vertebra below. This forward slippage is caused by a problem or defect within the pars interarticularis. Occasionally, facet joint and/or posterior neural arch defects may also cause this syndrome as well. The forward slippage does NOT always occur. This non-slipped pars defect is called a "Spondylolysis" and is almost always a precursor to the actual forward slippage.
Developmental anatomy • The first theory proposed a failure of ossification during embryonic development, leading to a pars interarticularis defect at birth • The second theory demonstrated that the pars defect began to appear around age six and became progressively more common till age 16. After age 16, the incidence fell and rarely developed after adolescence • It is currently thought that the defect develops from small stress fractures that fail to heal and form a chronic nonunion.
Classification • Dysplastic spondylolisthesis • Isthmic spondylolisthesis • DEGENERATIVE SPONDYLOLISTHESIS • TRAUMATIC SPONDYLOLISTHESIS • PATHOLOGICAL SPONDYLOLISTHESIS • IATROGENIC SPONDYLOLISTHESIS
Dysplastic spondylolisthesis • Is a true congenital spondylolisthesis that occurs because of malformation of the lumbosacral junction with small, incompetent facet joints. • Very rare, but tends to progress rapidly • Often associated with more severe neurological deficits.
Isthmic spondylolisthesis SUB-TYPE A: • Is the most commonly found type of spondylolisthesis in people under 50 years of age. • It is believed that "biomechanical stress," such as repetitive mechanical strain from heavy work or sports, causes a fatigue fracture within the pars interarticularis.
Isthmic spondylolisthesis SUB-TYPE B: • This type of Isthmic spondylolisthesis is characterized by a elongated pars without separation. • It is believed that the elongation occurs secondary to "repeated, minor trabecular stress fractures of the pars." Each time these possible sub-acute stress fractures occur and heal, the vertebral body is displaced farther and farther forward. Eventually, the pars may fail to heal and result as a full pars defect. SUB-TYPE C: These types of spondylolisthesis' are extremely rare and result from an acute pars fracture, often as result of traumatic lumbar hyperextension injury
DEGENERATIVE SPONDYLOLISTHESIS • This is the most common form of spondylolisthesis in patients over 50 years of age and rarely occurs in those under 50 • There is no fracture or elongation of the pars interarticularis and the neural arch is intact. In contrast, patients with isthmic spondyolisthesis almost universally have widening of the central spinal canal at the level of the slip. This narrowing of the canal in degenerative spondylolisthesis has been termed the "napkin ring effect.
DEGENERATIVE SPONDYLOLISTHESIS • The classic symptomology of patients with symptomatic degenerative spondylolisthesis are similar to those with symptomatic lumbar spinal stenosis; which can be either neurogenic claudication or radiculopathy (either unilateral or bilateral radiculopathy) with or without low back pain. • Neurogenic claudication is thought to result from central canal narrowing that is exacerbated by the listhesis (forward slip). The classic symptoms of neurogenic claudication are bilateral (both legs) posterior leg pain that worsens with activity, but is relieved by sitting or forward bending.
TRAUMATIC SPONDYLOLISTHESIS • This type of spondylolisthesis, which is extremely rare, results from a traumatically-induced fracture to the neural arch other than the pars region. • One of the examples is The "Hangman's Fracture" in the cervical spine's second vertebra (Axis) is a common and often deadly example of such a traumatically induced phenomenon. This type of fracture is extremely rare in the lumbar spine.
PATHOLOGICAL SPONDYLOLISTHESIS Generalized or systemic disorders of bone may affect the neural arch of the spine and allow spondylolysis or spondylolisthesis to occur. • Osteoperosis • Paget's disease • Metastatic carcinoma
IATROGENIC SPONDYLOLISTHESIS : • Is a complication of lumbar anterior interbody fusion (LAIF. Either the vertebrae above o below develops a pars fracture. • Laminectomy procedures will result in an overload of weight-bearing stress on the contralateral pars and, in some patients, result in a pars fracture.
symptoms • Spondylolysis commonly is asymptomatic. • Symptomatic patients often have pain with extension and/or rotation of the lumbar spine. • Common nerve symptoms
symptoms • Leg pain • Electric shock-like symptoms traveling down the leg • Numbness or tingling in the legs and feet • Muscle weakness of the legs • Other symptoms can occur. bowel or bladder dysfunction, or any numbness around the genitals, These symptoms may be a sign of cauda equina syndrome.
Limitations of Techniques • Radiography of the lumbar spine is limited by its inability to detect stress reactions in the pars interarticularis that have not progressed to complete fracture. • CT of the lumbar spine is not sensitive for detecting early acute stress reactions in the pars interarticularis where there is only marrow edema and microtrabecular fracture. • MRI of the lumbar spine can easily identify acute stress reactions in the pars interarticularis. However, direct identification of pars defects (old stress) may be slightly more difficult with MRI than with CT. • BONE SCAN : easily identifies acute stress reaction in the pars interarticularis, but cannot identify old pars defect.
Treatment • If the slip is small and the symptoms are manageable, then treatment is most often with observation. In children, this may include activity restrictions, such as withholding the child from participation in some sports. • When the slip is more significant, there may be a higher risk of the problem progressing, and surgery may be favored. In addition, patients who have symptoms of nerve compression are more likely to have surgery recommended.
Disorders of the neck • Torticollis • Klippel-Feil syndrome
Torticollis Definition Is a condition in which the head is tilted toward one side, and the chin is elevated and turned toward the opposite side.
Types of torticollis • Infantile torticollis • Acquired torticollis
Infantile torticollis • causes: • Birth trauma or intrauterine malposition • Sometimes a mass (a sternomastiod tumor) in the affected muscle may be noted, this appears at the age of two to four weeks, it disappears gradually, but sometimes the muscle becomes fibrotic. It is likely to disappear within the first five to eight months of life. • Other less common causes such as tumors, infections, ophthalmologic problems and other abnormalities should be ruled out. For example, ocular torticollis due to cranial nerve IV palsy. In this situation, the torticollis is a neurologic adaptation designed to maintain binocularity.
Infantile torticollis • treatment: • If a child has sternomastoid tumor, subsequent deformity may be prevented by gentle, daily manipulation of the neck. In established cases, the sternomastoid can be divided or elongated • Ocular torticollis due to cranial nerve IV palsy should not be treated with physical therapy. Rather the treatment should be targeted at the extraocular muscle imbalance
Acquired torticollis • causes: • Acute disc prolapse (the most common cause in adults) • Inflamed neck glands • Vertebral infection • Injuries of the cervical spine • Ocular disorders
Klippel-Feil syndrome • It is caused by a failure in the normal segmentation or division of the cervical vertebrae during the early weeks of fetal development.
Klippel-Feil syndrome • The most common signs of the disorder are short neck, low hairline at the back of the head, and restricted mobility of the upper spine.
Klippel-Feil syndrome • Treatment is symptomatic and may include surgery to relieve cervical instability and constriction of the spinal cord, and to correct scoliosis. Physical therapy may also be useful.