Download
1 / 1
10 likes | 134 Views
METHODS Number of patients : fixed sample size: 20 patients or Stopping rule approach: ≤ 30 for 5 doses or ≤ 48 patients for 8 doses, until the toxicity rate at the MTD is within (10% - 35%) Clinical outcome : Dose Limiting Toxicity (yes/no)

E N D
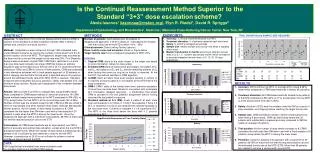
METHODS • Number of patients: fixed sample size: 20 patients or • Stopping rule approach: ≤ 30 for 5 doses or ≤ 48 patients for 8 doses, until the toxicity rate at the MTD is within (10% - 35%) • Clinical outcome: Dose Limiting Toxicity (yes/no) • Dose- toxicity curve and scenarios: shown in Figure below. • Target toxicity rate that is considered acceptable at MTD: 25% • DESIGNS • Original CRM: starts at the dose closest to the target rate based on prior information; allows for dose jumps. • Extended CRM starts at lowest dose and assigns one patient at D1 and D2, two patients at D3 and D4, and the remaining patients at D5 when testing five levels as long as no toxicity is observed. At the first DLT, the method switches to CRM algorithm. • G-CRM: starts at lowest dose level; assigns patients in cohorts of 3; requires at least 6 patients to be treated at the MTD before the study completion. • CRM-I: CRM-I starts at the lowest dose level, prevents escalation of more than one dose level. Allows for one patient with incomplete DLT information (delayed response) - a modification that allows CRM to proceed to the next patient’s assignment without having observed the last patient’s response. • Standard method of 3+3 (SM): treats 3 patients at each dose level and expands to 6 if there is 1/3 DLT, de-escalates if there ≥ 2 DLT, or otherwise if no DLT’s are observed the method escalates to the next dose level. Continue to escalate if ≤ 1/6 experience DLT. The MTD is the dose level below the dose with ≥ 2 patients experiencing DLT. CRM / E-CRM/ 20 20 20 20 20 20 20 20 CRM-I G-CRM 18 18 18 27 27 27 18 21 SM 18 18 18 27 27 27 12 18 • RESULTS • Accuracy: SM found the true MTD on average 20% (range 8-28%) fewer times compared to CRM-based methods in almost all scenarios. • Treatment allocation: All CRM-based methods treated more patients at the MTD compared to SM (42% vs 11%) except when the true MTD is at the second dose level (36 vs 35%). • Safety: Number of DLTs was the smallest under the SM as a result of slow escalation and stopping before reaching the target toxicity rate. • Sample size: CRM and SM are similar in terms of total sample size when testing 5 dose levels. CRM can test 8 dose levels with 20 patients with substantially increased accuracy compared to SM that needs on average 27 patients. • Trial duration: As the number of dose levels increases to 8, CRM-I completes the trial faster than SM when used with a fixed sample of 20 patients; except when the MTD is among the lower levels. • Precision: Using the stopping rule approach with a maximum of 30 patients, 66-78% of trials have not met the required precision around the estimated toxicity rate at the MTD (ETR). More than 36 patients are needed to achieve a narrow width around ETR. Treatment allocation 60 50 CRM 40 CRM-I % patients treated at MTD 30 E-CRM G-CRM 20 SM 10 0 1 2 3 4 5 6 7 8 Scenarios Is the Continual Reassessment Method Superior to the Standard “3+3” dose escalationscheme? Alexia Iasonos1 (iasonosa@mskcc.org), Elyn R. Riedel1, David R. Spriggs2 Department of Epidemiology and Biostatistics1, Medicine2, Memorial Sloan-Kettering Cancer Center, New York, NY ABSTRACT Objective: To determine if the Continual Reassessment Method (CRM) is superior to the standard 3+3 dose escalation scheme (SM) in terms of sample size, precision and study duration. Methods: Comparisons were carried out through 1000 simulated trials under different scenarios by varying the number of dose levels from 5 to 8 and the location of the true MTD. The hyperbolic tangent was assumed as the dose-toxicity curve and the target toxicity rate was 25%. Four Bayesian designs were evaluated: original CRM; CRM that is restricted in no more than one dose level increase; two-stage CRM that follows an arbitrary escalation plan at the beginning of the trial until a DLT is observed and then switches to CRM; and CRM in cohorts of three patients. CRM was assessed in two alternative schemes: with a fixed sample approach of 20 patients or with a stopping rule that halts the trial when a specified amount of precision around the estimated toxicity rate at the MTD (ETR) is reached. Standard endpoints were evaluated: accuracy, precision, safety, total sample size, and minimum study duration. Results are independent of the increment between dose levels. Results: SM found the true MTD on average 20% (range 8-28%) fewer times compared to CRM-based methods in almost all scenarios. All CRM-based methods treated more patients at the MTD compared to SM (42% vs 11%) except when the true MTD is at the second dose level (36 vs 35%). Number of DLTs was the smallest under the SM. CRM and SM are similar in terms of total sample size when testing 5 dose levels, although SM requires shorter duration. As the number of dose levels increases to 8, CRM completes the trial faster than SM when used with a fixed sample of 20 patients; except when the MTD is among the lower levels. Using the stopping rule approach with a maximum of 30 patients, 66-78% of trials have not met the required precision around the ETR. Conclusions: All CRM-based methods are an improvement over SM in terms of accuracy and optimal dose allocation, except when the true MTD is among the lower levels. When the number of dose levels is limited (eg ≤5), a sample of 20 is sufficient by both methods in order to find the MTD. However, a sample size of 20-30 is not sufficient to achieve a narrow confidence interval around the ETR. • ENDPOINTS • Accuracy: % of trials recommending the true MTD • Treatment allocation: % of patients treated at each dose level • Safety: % of DLT’s averaged across trials • Sample size: median sample size across trials when a stopping rule is used • Median trial duration in months assuming 4 different accrual rates of 3, 2, 1.5, 1 patient accrued per month, which correspond to average interpatient arrival times of 10, 15, 20, 30 days respectively. TRIAL DURATION and SAMPLE SIZE REQUIRED DATA 1000 hypothetical (simulated) trials were evaluated under the standard method and modified CRM designs.