Download
1 / 97
1.02k likes | 1.27k Views
Learn about proximal tibial fractures including anatomy, mechanism of injury, classifications, and surgical indications. Case examples and complications are also discussed.

E N D
台灣骨科創傷醫學會103年度住院醫師研習課程 Proximal Tibial Fractures Kai-Cheng Lin 高雄榮總骨科部 林楷城 103/08/16 台中榮總
Outlines • Anatomy • Mechanism of Injury • Examination/Evaluation • Classifications • Surgical Indications • Case Examples • Complications
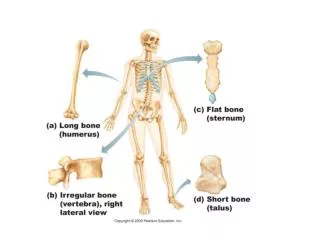
Anatomy of the Tibial Plateau • Proximal Tibia • Made up of medial and lateral plateau or condyles • Bony prominences (attachments) • Intercondylar eminence (ACL) • Tibial tubercle (Patellar Tendon) • Gerdy’s tubercle (ITB) • Joints • Knee joint (Distal Femur/Patella) • Proximal tib/fib joint
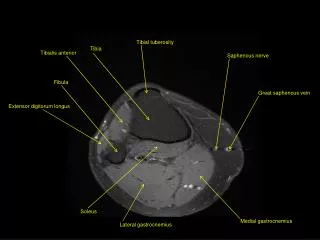
Anatomy of the Tibial Plateau • Medial Plateau • Concave • Larger • Cartilage thick ~ 3 mm • Posterior slope of 10° • Lateral Plateau • Convex • Higher on lateral view • Larger meniscus • Cartilage thick ~ 4 mm • Posterior slope of 7° MCL, ACL, LCL, Popliteal artery, peroneal nerve are all potentially at risk for injury
Meniscus • Lateral meniscus • More circular than medial • Covers more of articular surface than medial • Attached to PCL via ligaments • Humphry (anterior) • Wrisberg (posterior) • No attachment to LCL • Bears more joint reactive force • Medial meniscus • “C” shaped • intimately attached to MCL • bears equal joint reactive force as bone Lateral meniscuc is vulnerable to injury after trauma
Mechanisms of Injury • The first consideration: a low- or high-energy mechanism – Low-energy: a fall from a standing height – High-energy: Motorcycle or motor vehicle collisions • Fracture-dislocations, involvement of the medial tibial plateau, and metaphyseal comminution
Evaluation • Prior to evaluating the injured limb, a thorough trauma evaluation should be performed • Many tibial plateau fractures occur in multiply injured patients, and ATLS protocols must be initiated in this setting • Visual inspection: soft-tissue swelling, open lacerations, and limb deformity • Complete neurologic examination - Common peroneal nerve: at particular risk for injury due to close to the fibular neck
Evaluation • Can be associated with a knee dislocation, especially with medial tibial plateau frx → vascular examination is critical – distal pulse palpation, assessment of the color and temperature of the foot, and obtaining ankle-brachial indices (ABI) – An (ABI) <0.9 warrants more invasive vascular studies
Soft-tissue status • significant and clinically, relevant information -- fracture blisters -- non-wrinkling skin -- openlacerations -- tense compartments -- ecchymosis is present Bony injury is static and the soft-tissue injury is dynamic and can evolve
Compartment syndrome -> fasciotomy Clinical Diagnosis No Hesitate if Doubt
Radiographic Evaluation • AP, Lateral (Including two joints) • Obliques (optional) • Internal rotation view • Shows postero-lateral fragment • Traction Films (better joint interpretation) • Defines fragments • Bridging Ex-fix can provide traction • CT scan with reconstruction • Obtain after ex fix if using • Axial • Coronal • Sagittal • Arteriography when necessary (or check ABI > 0.9) • MRI – unsuspected fxs or soft tissue injury
Soft Tissue Injury on MRI 103 acute TPFs Gardner MJ et al. The incidence of soft tissue injury in operative tibial plateau fractures: a magnetic resonance imaging analysis of 103 patients. J Orthop Trauma 2005;19:79-84
The lateral collateral ligament (fibular collateral ligament)
Urgent and Provisional Treatments • Cross knee Ex-Fix: 2 Schanz half pins in femur & 2 pins in tibia • Connected with multiple clamps and bars in the region of the knee • Avoid placing the clamp directly over the knee to allow radiographic visualization • Tibial pins should be distal enough to avoid interference with the definitive incisions and implants • Joint over-distraction may be detrimental to neurovascular structures
Temporary External Fixation Femur Anterior or Antero-Lateral Tibia Medial or Antero-Medial Draw Operative Incisions Place Outside Area of Injury
Operative tactics—spanning external fixation • Restores and maintains length • Restores axial alignment of leg • Improves position of bone fragments by ligamentotaxis • Reduces further soft-tissue embarrassment • Allows outpatient treatment
Fracture classification OTA Type A Extraarticular Type B Partial articular Type C Complete articular 41-A1 41-A2 41-A3 (Schatzker I−IV) x 41-B1 41-B2 41-B3 (Schatzker V−VI) 41-C1 41-C2 41-C3
Fracture classification—Schatzker Low energy trauma High energy trauma Type I Type II Type III Type IV Type V Type VI partial articular fractures complete articular fractures
3-Column classification • Column fracture—breakage of corresponding cortex (compression/tension fracture) • Localize the articular surface depression—approach to reduce • Pure depression of articular surface (Schatzker type III)—“zero column fracture”
Indications of Non Op • Stable to varus and valgus stress • Not affect the coronal plane limb alignment • Minimal articular displacement • Nonambulatory or medically unstable patients should be considered for nonsurgical treatment • The importance of early joint motion to minimize stiffness and improve the nutrition and health of he injured cartilage has been stressed
Key points of TPFs • Meniscal preservation is critical for long-term joint maintenance • A recent large series of bicondylartibial plateau fractures: more accurate articular reconstruction improved functional outcomes -Laboratory data: 1.5 mm of incongruity of the lateral tibial plateau, the contact stresses on the adjacent cartilage are approximately doubled -A threshold of 2 mm of articular step-off is used for surgical indications and for intraoperative reductions
Surgical Goals of TPF Obtain/Secure Articular Reduction Reduce Condylar Width Restore Axial Alignment Neutralize Meta-Diaphysis Early ROM Appropriate Soft Tissue Handling Direct Visualization Arthroscopic aid Reduce Joint Depression Reserve Meniscus Restore Alignment Repair Ligamentous Stability Radiographically Medial/Lateral Plates Lateral Plate/Medial ExFix Lateral Fixed-Angle Plate External Fixation Hybrid
A new way of thinkingMorphology+injury mechanism Varus + extension Valgus + extension Flexion
Principles for approach selection • Biomechanical fixation • Touch of depressed articular fragment • Soft tissue tolerance
Principle for plate fixation • Buttress fixation is preferred for column fractures • Main buttress plate is chosen according to the injury mechanism • Bridging is used for comminuted metaphyseal fractures
Surgical Approaches • Straight Midline • Lateral Parapatellar • Medial Parapatellar • Posteromedial • Posterior • Dual approaches for bicondylar fractures • AVOID Mercedes incision or midline with stripping of soft tissues, especially for bicondylar fractures
Approaches Anterolateral Posteromedial
Anterolateral approach Check Meniscus
Partial articular fractures Schatzker type I Schatzker type II Schatzker type III Schatzker type IV
Schatzker type I • Split fracture • Open vs percutaneous treatment • Lag screws+/- buttress plate
Schatzker type II • Split depression fracture • Submeniscal arthrotomy • Elevation/bone graft • Lag screws/buttress plate
Schatzker III • Pure depression fracture • Amenable to percutaneous techniques with fluoroscopy +/- arthroscopy • Metaphyseal window for elevation and grafting • Screws beneath subchondral bone
Schatzker III Elevate the depressed central fragment from below
Type III Depression—preoperative 31-year-old
Arthroscopic Reduction IF medial depression fragment elevation
Fixation Lateral Plateau Fractures • Traditional • large fragment “L” or “T” buttress plate • 6.5mm subchondral lag screws • 4.5mm diaphyseal screw • Current Recommendation • small fragment fixation • pre-contoured peri-articular plates • clustered sudchondral k-wires • “rafting”
BiomechanicsSubchondral Fixation • 3.5 mm raft construct allowed significantly less displacement than 6.5 mm screw with axial load (2954 vs. 968 newtons/mm) Twaddle et al AAOS, 1997 • No difference in pull out strength between 6.5mm screws and 3.5mm screws in subchondral bone Westmoreland et al J Ortho Trauma 2002 • Subchondral clustered K-wires significantly enhance load tolerance to depression of articular surface Beris et al Bull Hosp Joint Dis 1996
Schatzker type IV • Medial tibial plateau fracture • Frequently realigned knee dislocations • Associated with: -Peroneal nerve injury 5 − 50% -Popliteal artery injury 13 − 50%