Download
1 / 64
650 likes | 1.07k Views
Closed Fractures of the Tibial Diaphysis. David L. Rothberg, MD Erik N. Kubiak, MD University of Utah Original Authors: Robert V. Cantu, MD and David Templeman, MD; March 2004 Interim Authors: David Templeman and Darin Friess, MD; Revised June 2006

E N D
Closed Fractures of the Tibial Diaphysis David L. Rothberg, MD Erik N. Kubiak, MD University of Utah Original Authors: Robert V. Cantu, MD and David Templeman, MD; March 2004 Interim Authors: David Templeman and Darin Friess, MD; Revised June 2006 New Authors: David L. Rothberg, MD & Erik N. Kubiak, MD; Revised June 2010
Tibia Fractures Most common long bone fracture 492,000 fractures yearly Average 7.4 day hospital stay 100,000 non-unions per year
History & Physical • Low Energy • Minimal soft-tissue injury • Less complicated fracture pattern and management decisions • 76.5% closed • 53.5% mild soft-tissue energy
History & Physical • High Energy • High incidence of neurovascular energy and open injury • Low threshold for compartment syndrome • Complete soft-tissue injury may not declare itself for several days
Radiographic Evaluation • Full length AP and Lateral Views • Check joint above & below • Oblique views may be helpful in follow-up to assess healing
Injuries Associated • 30% of patients will have multiple injuries • Ipsilateral Fibula Fracture • Foot & Ankle injury • Syndesmotic Injury • Ligamentous knee injuries
Injuries Associated • Ipsilateral Femur Fx • “Floating Knee” • Neurovascular Injury • More Common In: • High Energy • Proximal Fracture • Floating Knee • Knee Dislocation
Classification • Numerous systems • Important variables • Fracture Pattern • Location • Comminution • Associated Fibula Fx • Degree of soft-tissue injury
OTA Classification • Follows Johner & Wruh system • Describes relationship between fracture pattern & mechanism • Comminution is prognostic for time to union
Henley’s Classification • Applies Winquist & Hansen Femur classification to fractures of the Tibia
Tscherne Classification of Soft-Tissue Injury • Grade 0 • negligible soft tissue injury • Grade 1 • superficial abrasion or contusion • Grade 2 • deep contusion from direct trauma • Grade 3 • Extensive contusion and crush injury with possible severe muscle injury, compartment syndrome
Compartment Syndrome • Incidence: • 5-15% • History • High-Energy • Crush • Exam • 4 Compartments • 6 P’s • Pain • Pain with passive stretch • Parasthesias • Pulsless • Pallor • Paralysis
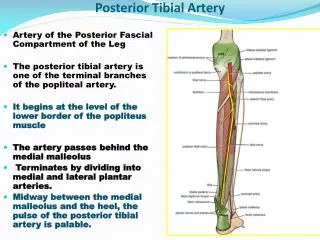
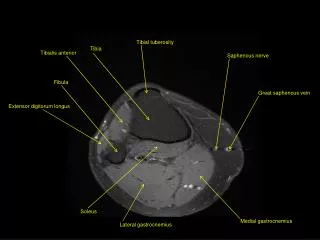
Compartment Anatomy • Anterior • Deep Peroneal N. • Lateral • Sup. Peroneal N. • Deep Post. • Tibial N. • Sup. Post. • Sural N.
Anterior Compartment • Action • Ankle dorsiflexion • Muscles • Tib. Ant. • EDL • EHL • Peroneus Tertius • Vessels • Anterior Tibial A./V. • Nerves • Deep Peroneal N.. • 1st webspace sensation
Lateral Compartment • Action • Foot Eversion • Muscles • Peroneus Brevis & Longus • Nerves • Superficial Peroneal N. • Dorsal foot sensation
Deep Posterior • Actions • Ankle plantarflexion • Foot inversion • Muscles • FDL • FHL • Tib. Post. • Vessels • Post Tibial A./V. • Peroneal A. • Nerve • Tibial N. • Plantar foot sensation
Superficial Posterior • Action • Ankle Plantarflexion • Muslces • Gastrocnemius • Soleus • Popliteus • Plantaris • Vessels • Greater and Lesser Saphenous V. • Nerve • Sural N. • Lateral heel sensation
Pressure Measurements • May be helpful in borderline cases • Basic Science • Muscle ischemia present at 20 mmHg below DBP and 30 mmHg below MAP • Various Thresholds • P = 30 mmHg • P = 45 mmHg • Whiteside’s Theory • ∆ P = DBP – CP = < 30 mmHg
Pressures Not Uniform • Highest at Fracture Site • Highest Pressures in: • Deep Posterior • Anterior • Heckman JBJS ’76 + ++ +++ ++ +
Clinical Monitoring • Close Observation • Repeat Exams • Repeat Pressure Measurements • Indwelling Monitors • Reserved for intubated patient with high suspicion
Goals of Fasciotomy • Decompress the compartment • Minimize further soft-tissue damage • Single vs. Two incisions • Go long • No increased morbidity • No difference in long-term outcome • Plan for fracture fixation • Plan for wound closure • Coordinate with location of future incisions and/or internal fixation
Closed Tibial Shaft Fracture • Broad Spectrum of Injures w/ many treatments • Closed Management • Intramedullary Nails • Plates • External Fixation
Non-Operative Treatment Indications • Minimal soft tissue damage • Non-intact fibula • Higher rate of nonunion & varus with intact fibula • Stable fracture pattern • < 5°varus/valgus • < 10° pro/recurvatum • < 1 cm shortening • Ability to bear weight in cast or fx brace • Requires frequent follow-up • Schmidt ICL 52, 2003
Fracture Brace • Closed Functional Treatment • 1,000 Tibial Fractures • 60% Lost to F/U • Fracture Characteristics • All < 1.5cm shortening • Non with intact fibula • Only 5% more than 8°varus • Treatment Course • Average 3.7 wks in long leg cast • Transition to Function Fracture Brace • Sarmiento JBJS ‘84
Sarmiento • Union Rate • 98.5% • Time to Union • 18.1 weeks • Shortening • <1.4% • Initial Shortening = Final Shortnening
Natural History • Long-term angular deformities • Well tolerated without associated knee or ankle arthrosis • Kristensen 22 pt F/U: 20-29 yrs • All patients >10 degree deformity • No radiographic Ankle arthrosis • Merchant & Dietz 37 pt F/U: 29 yrs • 76% of Ankles had G/E radiographic results • 92% of Knees had G/E radiographic results
Post Tibia Fracture Ankle Motion • 25% Post Tibia Fracture will lose 25% of Ankle ROM
Surgical Indications • Patient Characteristics • Obesity • Poor compliance with non-operative management • Need for early mobility • Injury Characteristics • High Energy • Moderate soft-tissue injury • Open Fracture • Compartment Syndrome • Ipsilateral Femur Fx • Vascular Injury • Fracture Characteristics • Meta-Diaphyseal location • Oblique fracture pattern • Coronal Angulation > 5° • Sagittal Angulation > 10° • Rotation > 5° • Shortening > 1cm • Comminution > 50% cortical circumference • Intact fibula
Surgical Options • Intramedullary Nail • ORIF with Plate • External Fixation • Combination of fixation
Advantage of IM Nail • Less malunion • Early weight-bearing • Early motion • Early WB (load sharing) • Patient satisfaction • L Bone, JBJS • Cost • Less expensive to society when compared to casting • Busse Acta Ortho ‘05
Disadvantages of IM Nail • Anterior knee pain • 2/3, improve w/in year • Risk of infection • Increased hardware failure with unreamed nails • Thermal Necrosis • Medial HW prominence
IM Nails • PRCT 62 pts • If displacement >50% angulation >10° • Nails superior to cast treatment Hooper JBJS-B ‘91
IM Nails – Bone et.al. Retrospective review 99 patients CastNail Time to union 26 wks 18 wks SF-36 74 85 Knee score 89 96 Ankle score 84 97 Bone JBJS ‘97
Reamed vs. Nonreamed Nails • Reamings (osteogenic) • Larger Nails (& locking bolts) • Hardware failure rare w/ newer nail designs • Damage to endosteal blood supply? • Clinically proven safe even in open fx Forster Injury ‘05 Bhandari JOT ‘00
Reamed vs. Nonreamed Nails Blachut JBJS ‘97 ReamedNon-Reamed # pts. 73 63 Nonunion 4% 11% Malunion 4% 3% Broken Bolts 3% 16% Time to Union 16.7 wks 25.7 wks Larsen JOT ‘04
IM Nails – Interlocking Bolts • Loss of alignment w/o interlocking • Spiral 7/22 • Transverse 0/27 • Metaphyseal 7/28 Templeman CORR ‘97
Infection 1-5% Union >90% Knee Pain 56% w/ kneeling 90% w/ running 56% at rest 33% Complications Court-Brown JOT ‘96
Knee Pain after IMN • Incidence • Varied in lit. 10-86% • Attributed to: • Skin Incision • Approach • Insertion Site • Quad weakness • Nail Prominence • Removal • 27% resolved • 69% marked improvement • 3% worse Court-Brown JOT ‘96
Neurologic Complications • 63 pts – compared types of anesthesia • Epidural Anesthesia • 4.1 x greater risk of neurologic injury • Illustrates need to monitor post-op exam • Iaquinto Am J Orth ‘97
Expanded Indications • Proximal 1/3 fractures • Beware Valgus and Procurvatum • Distal 1/3 fractures • Beware Varus or valgus • Beware of intraarticular extension
Proximal Tibia Fracture • Entry site is critical • Reference • Lateral Tibial Spine
Too Low! Too Medial! Valgus Procurvatum
Semiextended Position • Neutralize quadriceps pull on proximal fragment • Medial parapatellar approach • subluxate patella laterally • Use handheld awls to gently ream through the trochlear groove Tornetta CORR ‘96
Hyperextended position • Pulls patella proximally to allow straight starting angle • Universal distractor Beuhler JOT ‘97
Blocking (Poller) Screws • Functionally narrows IM canal • Increases strength and rigidity of fixation • Place on concave side of deformity • 21 patients • All healed within 3-12 months • Mean alignment 1° valgus, 2° procurvatum Krettek JBJS ‘99
Technique • Screws placed on concave side of deformity • Proximal or distal fractures
Distal Tibial Fractures • Reduction before reaming • Distractor • Fibula plate/nail • Joy Stick • Calcaneal Traction
Universal Distractor Reduction Beuhler JOT ‘97