Download
1 / 12
140 likes | 643 Views
Corneal Cap Recurrence: New thoughts on Pterygium pathophysiology. Nigel Morlet FRANZCO, FRACS with Weng Ng FRANZCO , and Tersia Vermeulen FRCPath The authors have no financial interest in subject matter. The treatments used in this case are “off-label”.

E N D
Corneal Cap Recurrence:New thoughts on Pterygium pathophysiology. Nigel Morlet FRANZCO, FRACS with Weng Ng FRANZCO, and Tersia Vermeulen FRCPath The authors have no financial interest in subject matter. The treatments used in this case are “off-label”.
Difficult to define exactly pathophysiologically, usually just has a descriptive definition. Is it a degeneration, or just an inflammatory process? Is it a disease of Conjunctiva, Limbus or Tenon’s capsule? Does it represent a progression of Pingueculum? How is it distinguished from “psuedo-pterygium”? What is the aetiological process?? What is a Pterygium?“Resembles only itself”Townsend paraphrases Amsler
Does this really look like anything other than a Pterygium? When does Pingueculum really become a Pterygium, if at all?? There is more to Pterygium than just Limbal stem cell failure.
Body: the fibrovascular component over the sclera. Neck: where it crosses the limbus. Head: the fibrovascular component over the cornea. Cap or Grey-zone: the clear subepithelial component in front of the head. Îles de Fuchs Stocker’s Line: the iron deposition line in the epithelium in front of the head. What is a Pterygium?Description: Ooi JL et al AJO 2007 More recently Pterygium was classified by the UV photography appearance.
Îles de Fuchs ? These are small “island shaped” sub-epithelial fibrotic lesions in front of, but not connected to the Cap of the Pterygium. Often seen under or in advance of Stocker’s line. Sometimes associated with a “peninsular” that is connected to the Cap. The leading edge of the Cap may have an irregular or crenated apearance as a result.
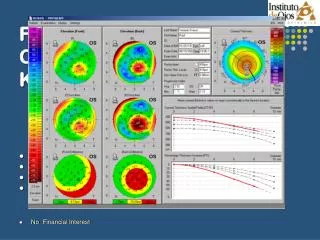
Pterygium Recurrence: An Illustrative Case • Dec 2004, Mr IP, 52 yo, presented c/o flare & diminished right visual acuity. • He had Ptergyium surgery 30 months prior, VA was ok initially, then gradually became worse over 12 to 24 months. • RVA with 6/15+ (20/45+). • Keratometry was difficult but had 7.0 to 8.5 D astigmatism WTR.
Recurrence:Initialmanagement • Feb 2005. • 20 % alcohol 25 - 30 seconds. • Lamellar dissection at the level of Bowman’s layer with a Took’s knife. • Silicone Hydrogel bandage contact lens dressing. Postoperative result March 2005 - RVA unaided 6/6 (20/20)! June 2005 - RVA unaided was 6/15+ (20/50), with glasses 6/9+ (20/30) By January the RVA with had deteriorated to 6/15+ (20/30). The corneal signs appeared just the same as before!
More Recurrence:Unusual case, differentmanagement • Second keratectomy • February 2007 • 20 % alcohol, 25 seconds. • Lamellar dissection at Bowman’s layer with a Took’s knife. • 50 mg/mL 5FU was applied for 5 minutes to stromal bed. • G. Interferon Alpha 2b 1x106 IU/mL qid was given postoperatively * The histopathology looked like a typical corneal stromal fibrotic scar. (pictures courtesy of Dr Tersia Vermeulen, histopathologist) * Morlet N, Gillies MC, Crouch R & Maloof A. Corneal Refractive Surgery 1993;9:443 - 451. see also, Esquenazi S Can J Ophthalmol 2005
Outcome: Yet more recurrence • March 2007 - unaided 6/5 (20/10). • June 2007 - Interferon drops ceased. • August 2007 still looking good. December 2007 – scar! Interferon drops were resumed.
Yet More Recurrence:Unusual case, differentmanagement again • Third keratectomy – March 2008. • 20 % alcohol 25 seconds. • Lamellar dissection at Bowman’s layer with a Took’s knife. • Mitomicin 0.02% was applied to the stroma for 30 seconds. • G. Interferon Alpha 2b 1x106 IU/mL qid before and after. • Interferon stopped in May 2008. • December 2009 – RVA unaided 6/7.5, with 6/5, no recurrence. • The left eye had the same problem! It was gradually getting worse whilst we concentrated on the right. However successful treatment the first time was achieved with a lamellar resection and the topical mitomycin/interferon combination. The histopathology looked the same as before.
Corneal Cap Recurrence:We found more cases when we looked • We have seen this recurrence develop 10 months to 26 years after Pterygium surgery in 8 other eyes. • The histopathology was the same in all cases.
The Lesson from Practice:New thoughts on the pathophysiology • Pterygium starts with a fibrosis that “percolates” out of the stroma forming “Islands”, these coalesce to form the Cap. • This attracts the fibrovascular Body across the limbus. • Led by the Isles, the Cap progresses centripetally, literally “dragging” the Body along behind. • The sub-epithelial scar looked just the same histopathologically in other cases we have excised similarly – eg sub-epithelial fibrosis from corneal graft wounds, Salzmanoid nodules, Cone nipples in keratoconus.