High flow nasal oxygen
High flow nasal oxygen. Mohammad Algendy ,MD Ain shams university. Concept …. The ability of nasal cannulae to provide positive pressure to the airways was first noted in neonates.

High flow nasal oxygen
E N D
Presentation Transcript
High flow nasal oxygen Mohammad Algendy ,MD Ain shams university
Concept … • The ability of nasal cannulae to provide positive pressure to the airways was first noted in neonates. • A similar continuous positive airway pressure (CPAP) effect, with higher flows, was noted in adults and from here, HFNOT developed.
The devices consist of nasal cannulae connected to • oxygen flow meter with an air–oxygen gas blender and gas analyser. • They offer gas flow rates of 40 - 60 litre/ min. • A heating system and humidifier allows delivery of gases at temperatures of between 33 &43°C and 95–100% humidity
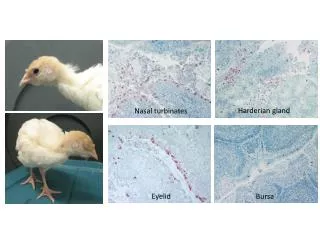
Physiological basis for the use of HFNOT • In health, quiet breathing generates gas flow =15 litre/ min. • this air is warmed and humidified in upper airway. • During nose breathing, this occurs through evaporation of water from nasal mucosa, with increased surface area by turbinates. • Gases reach a temperature of 36°C and humidification of 80–90% during passage through the upper airway. • Inhalation of air through mouth, however, reduces the maximum achievable R.humidity to 70%.
Physiological basis for HFNOT HFO & dead space
Physiological basis for HFNOT • HUMIDIFICATION & WARMING • HFNOT provides effective humidification & warming • of gases, which allows : • More effective clearance of secretions, • Decrease atelectasis. • Prevents airway surface dehydration.
Physiological basis for the use of HFNOT • HFNT provides an upper airway distending pressure of 3.2–7.4 cm H2O with mouth closed. • → Positive Airway Pressure • End-expiratory lung volume • Alveolar recruitment • Effect may be MORE IN higher body mass index.
Physiological basis for HFNOT WORK OF BREATHING • Splinting of the upper airway • → reducing airflow resistance in nasopharynx • thus reducing work of breathing.
ACUTE HYPOXEMIC RESPIRATORY FAILURE. • BRONCHOSCOPY . • POST-EXTUBATION & POSTOPERATIVE VENTILATION. • PREOXYGENATION. • IMMUNOCOMPROMIZED PATIENT. • COPD ?!!
prospective randomized crossover study in nonintubated patients with AHRF with PaO2/setFIO2 less than or equal to 300mmHgadmitted to the intensive care unit. applied HFNC set at 40 L/min compared with a standard nonocclusive facial mask at the same clinically set FIO2 (20 min/step)
total of 310 patients The intubation rate (primary outcome) was 38% (40 of 106 patients) in the high-flow–oxygen group, 47% (44 of 94) in the standard group, and 50% (55 of 110) in the noninvasive-ventilation group (P = 0.18 for all comparisons)
The number of ventilator-free days at day 28 was significantly • higher in the high-flow–oxygen group (24±8 days, vs. 22±10 in the standard- oxygen group and 19±12 in the noninvasive-ventilation group; P = 0.02
527 patients Patients were randomized to undergo either high-flow or conventional oxygen therapy for 24 hours after extubation.
retrospective observation study of critically ill patients older than 18 years who underwent intubation after HFNC failure and were treated in the ICU of Asan Medical Center, Korea, patients with HFNC failure were divided into early and late groups based on whether intubation started before or after 48 h HFNC initiation
TAKE HOME MESSAGE • High-flow nasal oxygen therapy (HFNOT) provides a valuable triad of Humidity. • High FIO2. • Improved patient compliance. • It reduces heat and moisture loss from the airway, reduces anatomical dead space, provides PEEP, and improves oxygenation.
TAKE HOME MESSAGE • There is increasing evidence for its use in acute respiratory failure, as an aid to preoxygenation, in the management of the difficult airway. • HFNOT can be useful in preventing postoperative respiratory failure. • Cautions for its use are similar to those for non-invasive facemask PPV.