Download
1 / 93
1.01k likes | 1.32k Views
Type I Diabetes Prevention. Ronen Gurfinkel , PGY5 April 3, 2013. Objectives. Review the pathogenesis of T1DM Review the prediction of T1DM Review studies on prevention of T1DM. Pathogenesis of T1DM. Autoimmune destruction of beta cells Occurs in susceptible individuals

E N D
Type I Diabetes Prevention Ronen Gurfinkel, PGY5 April 3, 2013
Objectives • Review the pathogenesis of T1DM • Review the prediction of T1DM • Review studies on prevention of T1DM
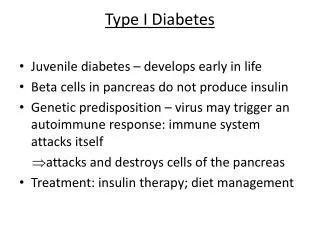
Pathogenesis of T1DM • Autoimmune destruction of beta cells • Occurs in susceptible individuals • Multiple polymorphisms known to influence risk (HLA and others) • Probable environmental triggers • Multiple autoantigen targets involved • Insulin, GAD65, IA-2, ZnT8 • Progresses over months-years • Long latent period
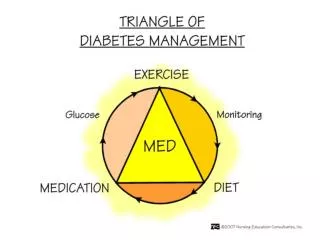
Stages of T1DM • Genetic susceptibility • Triggering of autoimmunity • Appearance of islet cell antibodies • Progressive loss of islet β cells with metabolic abnormalities • Complete loss of islet β cells and overt hyperglycemia
ENVIRONMENTAL TRIGGER (?) BETA CELL MASS GENETIC PREDISPOSITION INSULITIS BETA CELL INJURY “PRE”-DIABETES DIABETES TIME Natural History of Type 1 Diabetes CELLULAR (T CELL) AUTOIMMUNITY HUMORAL AUTOANTIBODIES (ICA, IAA, Anti-GAD65, ICA512 Ab, ZnT8A) LOSS OF FIRST PHASE INSULIN RESPONSE (IVGTT) GLUCOSE INTOLERANCE (OGTT) CLINICAL ONSET
T1DM Prediction • Need to identify high risk individuals • Increased efficiency of prevention trials • Interventions likely more effective if administered early in disease or prediabetic stages
T1DM Prediction • Genome-wide association study analyses have identified large number of genetic variants associated with T1DM • MHC HLA molecules are genetic determinants of T1DM • Class II alleles are a major determinant • DQ and DR molecules • Class I alleles are also a minor determinant
Human Leukocyte Antigens • HLA molecules present peptides to T cells • HLA molecules are made of 2 chains (heterodimers) • Each chain is coded by a separate gene • HLA molecules are very polymorphic
HLA Molcules • Class I – 3 major proteins • HLA A, HLA B, and HLA C • Class II – 3 major proteins • HLA-DP, HLA-DQ, and HLA-DR
HLA Class II • HLA-DP • α chain: HLA-DPA1 • β chain: HLA-DPB1 • HLA-DQ • α chain: HLA-DQA1 • β chain: HLA-DQB1 • HLA-DR • α chain: HLA-DRA • β chain: HLA-DRB1, DRB3, DRB4, or DRB5
MHC HLA • Nomenclature • Usually only polymorphic loci are specified (eg DRB chain, but not DRA chain) • Each variant designated with gene locus name followed by * • 2 digits referring to serologic specificity • 2 digits referring to specific allele (DNA-based typing) • eg DRB1*0405
MHC HLA • Groups of HLA alleles are usually inherited together, and referred to as haplotype • Two MHC haplotypes MHC genotype
HLA and T1DM Risk • Highest risk with DR3-DQ2 with DR4-DQ8 (DR3/4,DQ8/2) • 1 in 16 will develop T1DM • Children age 10 with T1DM: 50% have this genotype • 50% of offspring (of T1DM patients) with DQ2/8 will develop T1DM • 95% of all T1DM have either DR3-DQ2 or DR4-DQ8 • This is also present in 40% of general population
Diabetes Autoantibodies Zheng L and Eisenbarth GS. Prediction and prevention of Type 1 diabetes mellitus. Journal of Diabetes 2011; 3:48-57
Insulin Autoantibodies (IAA) Background: • Detected in new-onset T1D prior to insulin Rx • Insulin the only β-cell specific autoantigen so far • Indistinguishable from antibodies due to exogenous insulin therapy (~ 2 weeks of Rx insulin) New-onset T1D ~ 50 - 70% positive (esp. kids) Healthy controls < 3% positive
Glutamic Acid Decarboxylase 65 Antibodies (GAD65A) Background: • 64-kDa protein immunoprecipitated by mixing sera from kids with new-onset T1D with homogenized islets • Subsequently identified as GAD65 (high volume assays using recombinant GAD65) New-onset T1D ~ 70 - 80% positive Healthy controls < 3% positive
IA-2 Antibodies (IA-2A/ICA512) • Background: • Insulinoma-associated protein 2 • 40-kDa protein • Member of the protein tyrosine phosphatase family • Localized on the insulin granule membrane New-onset T1D ~ 50 - 75% positive Healthy controls < 2% positive
Antibodies and T1DM Prediction • Risk increases as number of antibodies present increases • 5-year risk in relatives of T1DM* • 2 antibodies 68% • 3 antibodies >90% • Antibodies have varying sensitivity for detecting T1DM • Testing for multiple antibodies will increase sensitivity *Verge CF et al. Prediction of type I diabetes in first-degree relatives using a combination of insulin, GAD, and ICA512bdc/IA-2 autoantibodies. Diabetes 1996; 45:926-33.
Future T1D Can Reliably Predicted in Persons with a Family History of T1D Number at Risk 1718 405 378 147 1401 297 255 95 1045 229 192 61 743 163 130 40 557 118 78 30 457 91 49 22 371 66 31 16 1 2 3 4 199 35 14 8 1.0 0.9 0.8 0.7 p-value < 0.001 (Log Rank Test) n = 26,799 0.6 0.5 Survival Distribution Function 0.4 0.3 0.2 0.1 0.0 0 1 2 3 4 5 6 7 8 Years Followed 1 2 3 4 No. Positive Abs:
Independent Predictors of T1D 20 yrs < 20 yrs 10th centile <10th centile Normal IGT ICA alone + 2 Ab + 3 Ab endit Age FPIR OGTT Islet antibodies + 1 Ab 1 10 100 Adjusted Hazard Ratio (95% CI)
Prediction of T1DM • Combination of • Family history (eg first-degree relatives) • Genetic markers (eg HLA class II & I) • Autoantibody markers • Metabolic markers (eg c-peptide, 2h-glucose, FPIR)
Erlich HA et al. Prediction of Type 1 Diabetes. Diabetes 2013; 62:1020-1021
T1DM Interventions • Primary intervention • Interval preceding detectability of disease • Secondary intervention • In presence of disease but asymptomatic and euglycemic preclinical phase • Tertiary intervention • Overt diabetes • Quaternary • Replacement of tissues/organs Dupré J and Mahon JL. Preventive Interventions for Type 1 Diabetes: History, Appraisal and Prospects. Can J Diabetes 2007; 31:384-394.
T1DM Tertiary Intervention • Basis for tertiary intervention • 10-20% of β-cells present at disease onset • Honeymoon phase from improved function of residual β-cells • “Rescuing” residual β-cells from immune destruction may improve clinical picture • Effective interventions in animal models (most are secondary prevention) lead to human trials • Nonobese diabetic (NOD) mouse • Biobreeding (BB) rat
Type 1 Diabetes Prevention in NOD Mice Mycobacterium avium Mycobacterium leprae Natural antibodies Natural polyreactive autoantibodies Neuropeptide calcitonin gene-related peptide Nicotinamide Nicotine Ninjin-to (Ren-Shen-Tang), a Kampo (Japanese traditional) formulation NKT cells NY4.2 cells OK432 Overcrowding Pancreatectomy Pentoxifylline Pertussigen Poly [I:C] Pregestimil diet Prenatal stress Preproinsulin DNA Probucol Prolactin Rampamycin Recombinant vaccinia virus expressing GAD Reg protein Reg protein Rolipram Saline (repeated injection) Schistosomamansoni Semi-purified diet (e.g., AIN-76) Short term chronic stress Silica Sirolimus/tacrolimus Sodium fusidate Soluble interferon-gamma receptor Somatostatin Non-specific pathogen free conditions Streptococcal enterotoxins Streptozotocin Sulfatide (3’sulfogalactosylceramide) Superantigens Superoxide dismutase-desferrioxamine Anti-T cell receptor TGF-beta 1 somatic gene therapy Th1 clone specific for hsp60 peptide Anti-thy-1 Thymectomy (neonatal) Tolbutamide Tolerogenic dendritic cells induced by vitamin D receptor ligands Top of the rack Treatment combined with a 10% w/v sucrose-supplemented drinking water Tumor necrosis factor-alpha TX527 (19-nor-14,20-bisepi-23-yne-1,25(OH)(2)D(3)) Vitamin E Anti-VLA-4 Gonadectomy Guanidinoethyldisulphide Heat shock protein 65 Heat shock protein peptide (p277) Hematopoietic stem cells encoding proinsulin Housing alone Human IGF-1 I-A beta g7(54-76) peptide Anti-I-A monoclonal antibodies Anti-ICAM-1 IgG2a antibodies Immobilization Inomide Anti-integrin alpha 4 Insulin (intraperitoneal, oral, subcutaneous, nasal) Insulin B chain (plasmid) Insulin B chain/B chain amino acids 9-23 (intraperitoneal, oral, subcutaneous, nasal) Insulin-like growth factor I (IGF-I) Anti-intercellular adhesion molecule-1 (ICAM-1) Interferon-alpha (oral) Interferon-gamma Anti-interferon-gamma Interferon-gamma receptor/IgG1 fusion protein Interleukin-1 Interleukin-4 Interleukin-4-Ig fusion protein Interleukin-4-plasmid Interleukin-10 Interleukin-10-plasmid DNA Interleukin-10-viral Interleukin 11-human Interleukin-12 Intrathymic administration of mycobacterial heat shock protein 65 Intrathymic administration of mycobacterial heat shock peptide p277 Islet cells-intrathymic L-Selectin (MEL-14) Lactate dehydogenase virus (LDH) Large multilamellar liposome Lazaroid Anti-leukocyte function associated antigen (LFA-1) Anti-LFA-1 Linomide (quinoline-3-carboxamide) Lipopolysaccharide-activated B cells Lisofylline Lymphocyte choriomeningitis virus (LCMV) Anti-lymphocyte serum Lymphoctyte vaccination Lymphocytic choriomeningitis virus Anti-L-selectin Lymphotoxin LZ8 MC1288 (20-epi-1,25-dihydroxyvitamin D3) MDL 29311 Metabolically inactive insulin analog Anti-MHC class I Anti-MHC class II MHC class II derived cyclic peptide Mixed allogeneic chimerism Mixed bone marrow chimeras Monosodium glutamate Murine hepatitis virus (MHV) AAV murine IL-10 AAV rat preproinsulin gene (vLP-1) Adenovirus expressing mIL-4 Aerosol insulin Allogenicthymic macrophages Alpha Galactosylceramide Alpha-interferon (rIFN-alpha) Alpha/beta T cell receptor thymocytes Aminoguanidine Androgens Anesthesia Antioxidant MDL 29,311 Antisense GAD mRNA Azathioprine Anti-B7-1 BacilleCalmetteGue’rin (BCG) Baclofen Bee venom Biolistic-mediated IL-4 Blocking peptide of MHC class II Bone marrow transplantation Castration Anti-CD3 Anti-CD4 CD4+CD25+regulatory T cells Anti-CD8 Anti-CD28 MAb Cholera toxin B subunit-insulin protein Class I derived self-I-A beta(g7) (54-76) peptide Cold exposure Anti-complement receptor Complete Freund’s adjuvant Anti-CTLA-4 Cyclic nucleotide phosphodiesterases (PDEs) Cyclosporin Cyclosporin A DC deficient in NF-kappaB DC from pancreatic lymph node DC with IL-4 Deflazacort Deoxysperogualin Dexamethasone/progesterone/growth hormone/estradiol Diazoxide 1,25 dihydroxy Vitamin D3, KH1060 1,25 dihydroxycholecalciferol 1,25 dihydroxyl Vitamin D3 Elevated temperature Emotionality Encephalomyocarditis virus (ECMV) Essential fatty acid deficient diets FK506 FTY720 (myriocin) GAD 65 peptides in utero Anti-GAD monoclonal antibody Galactosylceramide Glucose (neonatal) Glutamic acid decarboxylase (intraperitoneal, intrathymic, intravenous, oral) Glutamic acid decarboxylase 65 Th2 cell clone Glutamic acid decarboxylase peptides (intraperitoneal, intrathymic, intravenous, oral) 234 As of March, 2006
Tertiary Intervention • Insulin • Immunosuppression/Immunomodulation • Cyclosporin • Azathioprine • GAD65 (GAD65-alum) • Anti-CD3 antibodies • Anti-CD20 antibodies (Rituximab) • Other • Thymoglobulin • MMF • Sirolimus • BCG vaccine • Heat-shock protein 60-p277 peptide • Anti-CD25 antibody • Lisofylline • IFN-α2a
Insulin for T1DM Tertiary Intervention • Small studies showed aggressive insulin therapy early in T1DM improved β cell function • Shah et al, NEJM 1989 • 26 patients • Randomized to either • NPH 1 U/kg given BID • Continuous IV insulin infusion (target BG 3.3-4.4) x 2 weeks then usual care • At 1 year, IV insulin group had • Higher C-peptide level post mixed-meal • Better HbA1c (7.2% vs 10.8%) Shah et al, A Randomized Trial of Intensive Insulin Therapy in Newly Diagnosed Insulin-Dependent Diabetes Mellitus. N Engl J Med 1989; 320:550-554.
Insulin for T1DM Tertiary Intervention • DCCT, Ann Int Med 1998 • 855 (of 1441) T1DM 1-5 years at baseline • 303/855 were “C-peptide responders” • Randomized to intensive vs conventional treatment • Responders in intensive therapy group • Maintained higher stimulated C-peptide levels • Less likely to become “nonresponders” • Among intensive treatment in entire DCCT cohort responders had • Lower HbA1c • Lower rates of retinopathy • Lower risk of severe hypoglycemia DCCT Research Group. Effect of intensive therapy on residual beta-cell function in patients with type 1 diabetes in the diabetes control and complications trial. A randomized, controlled trial. Ann Intern Med. 1998 Apr 1;128(7):517-23.
Cyclosporin for T1DM Tertiary Intervention • Cyclosporin A prevented T1DM in rodents • Human pilot studies showed partial remission • Enhanced β cell function in 2 RCTs • CERT • CCF Study Group Diabetes
Canadian-European Randomized Control Trial Group • CERT Group, Diabetes 1988 • Recent T1DM (< 6 weeks) • 188 participants, age 9-35 • Randomized to cyclosporin or placebo • Cyclosporin 10 mg/kg/day given q12h • Titrated based on trough levels • Double-blinding for diabetes management • Unblinded management of cyclosporin • Target BGs ≤ 7.8 mM (ac meals and hs) • Insulin doses minimized • Stimulated C-peptide at 3-month intervals • Remission defined as: • Stim CP ≥ 0.6 mM • Non-insulin receiving (NIR) state CERT Group. Cyclosporin-lnduced Remission of IDDM After Early Intervention Association of 1 yr of Cyclosporin Treatment With Enhanced Insulin Secretion. Diabetes 1988;37:1574-82.
Canadian-European Randomized Control Trial Group CERT Group. Cyclosporin-lnduced Remission of IDDM After Early Intervention Association of 1 yr of Cyclosporin Treatment With Enhanced Insulin Secretion. Diabetes 1988;37:1574-82.
Canadian-European Randomized Control Trial Group CERT Group. Cyclosporin-lnduced Remission of IDDM After Early Intervention Association of 1 yr of Cyclosporin Treatment With Enhanced Insulin Secretion. Diabetes 1988;37:1574-82.
Cyclosporin/Diabetes French Study Group • CCF Study Group Diabetes, Lancet 1986 • Recent onset T1DM • 122 participants, age 15-40 • Randomized to cylcosporin or placebo • Cyclosporin 7.5 mg/kg/d • At 6 months • Complete remission 25.4% of cyclosporin group vs. 18.6% of placebo group • Treatment continued for partial/complete remission (n=106) • At 9 months • Complete remission 24.1% of cyclosporin group vs. 5.8% of placebo group CCF Study Group Diabetes. Cyclosporin Increases the Rate and Length of Remissions in Insulin-dependent Diabetes of Recent Onset: Results of a Multicentre Double-blind Trial. Lancet 1986;328:119-124
Azathioprine for T1DM Tertiary Intervention • Mixed results in newly diagnosed T1DM • Harrison LC et al, Diabetes 1985 • 24 patients, age 15-50 • Azathioprine 2 mg/kg showed benefit on basal and stim CP levels • Cook JJ et al, Diabetes 1989 • 49 patients, age 2-20 • Azathioprine 2 mg/kg did not give significant difference in remission rates, CP levels Harrison LC, Colman PG, Dean B, et al. Increase in remission rate in newly diagnosed type 1 diabetic subjects treated with azathioprine. Diabetes 1985;34:1306–1308. Cook JJ, Hudson I, Harrison LC, et al. A double-blind controlled trial of azathioprine in children with newly-diagnosed type 1 diabetes. Diabetes 1989;38:779–783.
Azathioprine for T1DM Tertiary Intervention • Silverstein, NEJM 1988 • Newly diagnosed T1DM (< 2 weeks) • 46 patients, age 4-32 • Randomized to azathioprine/prednisone or placebo • Prednisone x 10 weeks + azathioprine x 1 year • Unblinded study • “Satisfactory” outcome • HbA1c < 6.8%, stim CP > 0.5 mM, insulin dose < 0.4 U/kg/d Silverstein et al. Immunosuppression with Azathioprine and Prednisone in Recent-Onset Insulin-Dependent Diabetes Mellitus. N Engl J Med 1988; 319:599-604.
Azathioprine for T1DM Tertiary Intervention Silverstein et al. Immunosuppression with Azathioprine and Prednisone in Recent-Onset Insulin-Dependent Diabetes Mellitus. N Engl J Med 1988; 319:599-604.
Azathioprine for T1DM Tertiary Intervention • Silverstein, NEJM 1988 • “Satisfactory” outcome • HbA1c < 6.8%, stim CP > 0.5 mM, insulin dose < 0.4 U/kg/d • At 1 year • Satisfactory outcome in 50% of immunosuppressed group vs. 15% of placebo group Silverstein et al. Immunosuppression with Azathioprine and Prednisone in Recent-Onset Insulin-Dependent Diabetes Mellitus. N Engl J Med 1988; 319:599-604.
Anti-CD3 Ab for T1DM Tertiary Intervention • Targets CD3 receptors on T cells • Beneficial effects possibly by activation of regulatory T cells • ? selective deletion of activated Th1 cells and/or activation of Th2 cells and their protective cytokines • OKT3 reversed diabetes in nonobese diabetic (NOD) mice • Cytokine mediated side-effects • Humanized monoclonal antibodies developed • Teplizumab • Otelixizumab
Teplizumab [hOKT3γ1(Ala-Ala)] • Herold et al, NEJM 2002 • T1DM < 6 weeks • 24 patients, age 7-30 • Randomized to teplizumab or placebo • Teplizumab single 14-day course Herold et al. Anti-CD3 Monoclonal Antibody in New-Onset Type 1 Diabetes Mellitus. N Engl J Med 2002; 346:1692-1698.
Herold et al. Anti-CD3 Monoclonal Antibody in New-Onset Type 1 Diabetes Mellitus. N Engl J Med 2002; 346:1692-1698.
Herold et al. Anti-CD3 Monoclonal Antibody in New-Onset Type 1 Diabetes Mellitus. N Engl J Med 2002; 346:1692-1698.
Herold et al. Anti-CD3 Monoclonal Antibody in New-Onset Type 1 Diabetes Mellitus. N Engl J Med 2002; 346:1692-1698.
Teplizumab [hOKT3γ1(Ala-Ala)] • Herold et al, NEJM 2002 • At 1 year • Improved insulin production in 9/12 in teplizumab group vs. 2/12 in placebo group • Lower HbA1c and insulin doses in teplizumab group Herold et al. Anti-CD3 Monoclonal Antibody in New-Onset Type 1 Diabetes Mellitus. N Engl J Med 2002; 346:1692-1698.
Teplizumab (Protégé study) • Sherry N et al, Lancet 2011 • T1DM ≤ 12 weeks • 516 patients, age 8-35 • Randomized 2:1:1:1 ratio, double-blind • Teplizumab 14-day full dose, 14-day low dose, 6-day full dose, or placebo • Primary outcome: % patients at 1 year with both • Insulin dose < 0.5 U/kg/d • HbA1c < 6.5% Sherry N et al. Teplizumab for treatment of type 1 diabetes (Protégé study): 1-year results from a randomised, placebo-controlled trial. Lancet 2011; 378:487-97.
Teplizumab (Protégé study) Sherry N et al. Teplizumab for treatment of type 1 diabetes (Protégé study): 1-year results from a randomised, placebo-controlled trial. Lancet 2011; 378:487-97.
Teplizumab (Protégé study) • Subgroup analysis • Reduction in median AUC of CP was lower in treatment subgroups • Age 8-11 • Randomized < 6 weeks after diagnosis Sherry N et al. Teplizumab for treatment of type 1 diabetes (Protégé study): 1-year results from a randomised, placebo-controlled trial. Lancet 2011; 378:487-97.
Sherry N et al. Teplizumab for treatment of type 1 diabetes (Protégé study): 1-year results from a randomised, placebo-controlled trial. Lancet 2011; 378:487-97.
Otelixizumab (ChAglyCD3) • Keymeulen et al, NEJM 2005 • T1DM < 4 weeks • 80 patients, age 12-39 • Randomized to Otelixizumab or placebo • Otelixizumab single 6-day course Keymeulen et al. Insulin Needs after CD3-Antibody Therapy in New-Onset Type 1 Diabetes. N Engl J Med 2005; 352:2598-608