Download
1 / 15
300 likes | 2.59k Views
Management of Increased ICP. PICU Resident Talk Stanford School of Medicine Pediatric Critical Care Medicine June 2010. Objectives. After this lesson, the participant will be able to: Describe the principles of the Monro -Kellie Doctrine

E N D
Management of Increased ICP PICU Resident Talk Stanford School of Medicine Pediatric Critical Care Medicine June 2010
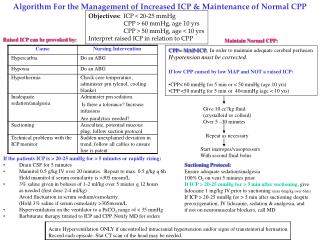
Objectives After this lesson, the participant will be able to: • Describe the principles of the Monro-Kellie Doctrine • Calculate cerebral perfusion pressure using MAP and ICP • List key management strategies for increased ICP
Basic Principles • Monro-Kellie Doctrine • The skull has a fixed volume • The skull contains • Brain matter • Cerebrospinal fluid • Blood • Therefore: An increase in the volume of one must be compensated by a decrease in the volume of the others or an increase in ICP will occur • Cerebral Perfusion Pressure • CPP = MAP - ICP
A mass will eventually cause an increase in ICP An ICP > 20 is associated with icreased morbidity and mortality
Aims of Management • Maintain cerebral perfusion pressure and support blood pressure • Decrease brain metabolism • Decrease the pressure!!
Hypotension is Associated with Worse Outcomes Kokoska. J Pediatr Surg. 1998 Feb;33(2):333-8.
Maintaining Adequate Brain Oxygenation • Maintain cerebral perfusion • Minimum CPP > 40 mmHg (PCCM guidelines) • Target CPP > 45-50 mmHg • Adult goal CPP > 65 mmHg • Decrease cerebral metabolism • Keep patient adequately sedated and analgesed • In extreme cases, use a pentobarbital induced coma
5 Ways to Decrease Intracranial Pressure Using the Monro-Kellie Doctrine • Enhance venous drainage • Elevate head 30° • If in a cervical collar, check fit • Hyperosmolar therapy • Hyperventilation • CSF Drainage • Decompression
Hyperosmolar Therapy • Goal is to increase serum osmolality to draw water out of brain parenchyma • Mannitol • 0.5 - 1g/kg • 3% Saline • Every 1.5 cc/kg will increase Na by ≈ 1 mEq/L • Known to have a longer lasting effect • In general, check Na2+ and osmolality q6h • Target Na2+ 150-160 • Target osmolality > 300
Hyperventilation Causes a Decrease in Cerebral Blood Flow PCO2 30 pCO2 45 Skippen. Crit Care Med. 1997 Aug;25(8):1402-9
Use of Hyperventilation • Worse long-term outcome • Target normocapnea • Works for acute spikes in ICP • Target pCO2 of about 35 • Avoid hypercapnea
CSF Drainage • Neurosurgical Procedure • Always push for an EVD, not just an ICP monitor • Therapeutic AND diagnostic • Can stay in long-term (no drift) • Requires INR < 1.5 and PLTS > 100K
Decompressive Craniectomy • Done infrequently • Usually done at an OSH prior to transfer OR in conjunction with hematoma evacuation • Remember to save the bone flap for reimplantation later http://www.rescueicp.com/Image533554-copy.jpg
Avoid the Bad “H”s • Hypotension • Hypoxia • Hyponatremia • Hypervolemia • Hyperglycemia • Hyperthermia • Hypermetabolism (seizures, agitation)
Summary of Key Points • Many of the goals of increased ICP management are based using the Monro-Kellie Doctrine to our advantage • Goal ICP < 20 mmHg • Hyperventilation is not a long-term strategy • CPP = MAP – ICP; Maintain CPP > 40 mmHg • Goal Na2+ 150-160 • Avoid the bad “H’s”