Download
1 / 1
50 likes | 293 Views
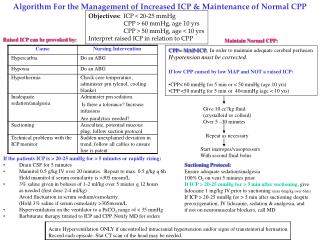
Algorithm For the Management of Increased ICP & Maintenance of Normal CPP. Objectives: ICP < 20-25 mmHg CPP > 60 mmHg, age 10 yrs CPP > 50 mmHg, age < 10 yrs Interpret raised ICP in relation to CPP. Raised ICP can be provoked by:. Maintain Normal CPP:.

E N D
Algorithm For the Management of Increased ICP & Maintenance of Normal CPP Objectives: ICP < 20-25 mmHg CPP > 60 mmHg, age 10 yrs CPP > 50 mmHg, age < 10 yrs Interpret raised ICP in relation to CPP Raised ICP can be provoked by: Maintain Normal CPP: • CPP= MAP-ICP. In order to maintain adequate cerebral perfusion • Hypotension must be corrected. • If low CPP caused by low MAP and NOT a raised ICP: • CPP< 60 mmHg for 5 min or < 50 mmHg (age 10 yrs) • CPP <50 mmHg for 5 min or 40<mmHg (age < 10 yrs) Give 10 cc?kg fluid (crystalloid or colloid) Over 5 –30 minutes Repeat as necessary Start inatropes/vasopressors With second fluid bolus • If the patients ICP is > 20-25 mmHg for > 5 minutes or rapidly rising: • Drain CSF for 5 minutes • Mannitol 0.5 g/kg IV over 20 minutes. Repeat to max. 0.5 g/kg q 6h • Hold mannitol if serum osmolarity is >305 mosm/L • 3% saline given in boluses of 1-2 ml/kg over 5 miutes q 12 hours • as needed (first dose 2-4 ml/kg) • Avoid fluctuation in serum sodium/osmolarity. • (Hold 3% saline if serum osmolarity >305mosm/L • Hyperventilation on the ventilator to a PaCO2 range of < 35 mmHg • Barbiturate therapy titrated to ICP and CPP. Notify MD for orders Suctioning Protocol: Ensure adequate sedation/analgesia 100% O2 on vent 5 minutes prior If ICP > 20-25 mmHg for > 5 min after suctioning, give lidocaine 1 mg/kg IV prior to suctioning (max 6mg/kg over 6hrs) If ICP > 20-25 mmHg for > 5 min after suctioning despite preoxygenation, IV lidocaine, sedation & analgesia, and if not on neuromuscular blockers, call MD Acute Hyperventilation ONLY if uncontrolled intracranial hypertension and/or signs of transtentorial herniation. Record each episode. Stat CT scan of the head may be needed.