Update Chelation Therapy
Chatdanai Musigchai, MD. Update Chelation Therapy. ปรัชญาของการแพทย์ทางเลือก. กำเนิดการแพทย์ทางเลือก

Update Chelation Therapy
E N D
Presentation Transcript
Chatdanai Musigchai, MD. Update Chelation Therapy
ปรัชญาของการแพทย์ทางเลือกปรัชญาของการแพทย์ทางเลือก • กำเนิดการแพทย์ทางเลือก จากการแพทย์พื้นบ้านของแต่ละประเทศ ที่ถูกเหยียบย่ำและเหยียดหยามจากการแพทย์ตะวันตกที่รุกเข้าครอบครองประเทศต่างๆพร้อมด้วยอำนาจปืนไฟ ในสมัยล่าอาณานิคม การแพทย์ตะวันตกเข้าแทน กลายเป็นการแพทย์กระแสหลัก: • การแพทย์แผนไทย -ไทย • การแพทย์แผนจีน -จีน • อายุรเวท –อินเดีย เมื่อการแพทย์ใช้ยาให้คำตอบไม่ได้ทั้งหมด ผู้คนจึงหันหาการแพทย์พื้นบ้าน
ปรัชญาของการแพทย์ทางเลือกปรัชญาของการแพทย์ทางเลือก • จากการคิดนอกกรอบของแพทย์ที่เคยอยู่ในระบบ • พัฒนาเป็นการแพทย์แนวทางใหม่ๆ • แมกโครไบโอติกส์ • เวชกรรมความคล้าย (โฮมิโอพาธีย์) • คีเลชั่น • อบความร้อน –hyperthermia • เซลล์บำบัด
ความเบี่ยงเบนแพทย์ทางเลือกปัจจุบันความเบี่ยงเบนแพทย์ทางเลือกปัจจุบัน • เชื่อพลังธรรมชาติน้อยลง เชื่อพลังบำบัดตัวเองน้อยลง • ผู้รักษาจำนวนมาก ยังมิได้ปฏิบัติด้วยตนเองตามแนวทางที่ตนจะรักษา • เน้นการปรับเปลี่ยนชีวิตน้อยลง ปชช.พึ่งตนเองน้อยลง • เน้นพึ่งแพทย์ วิตามิน การใช้เทคโนโลยีทางเลือกมากขึ้น • แม้ไม่ใช้ยาเคมี แต่ใช้วิตามินมากขึ้น ห่างไกลธรรมชาติยิ่งขึ้น • เป็นธุรกิจมากขึ้น ค่อนไปในทางเพื่อการค้ากำไรมากขึ้น • ราคาแพงขึ้น บางครั้งไม่คำนึงถึงข้อบ่งชี้ทางวิชาการ ใช้แบบครอบจักรวาล • เน้นปฏิบัติทางจิตใจน้อยลง บทบาททางจิตโน้มเอียงไปด้านใช้เครื่องมือ
He is considered one of the most influential chemists of the 20th century and ranks among the most important scientists in history. Nobel Prize Winner: Nobel Laureate TwiceProfessor of ChemistryUniversity of California Linus Carl Pauling
CHELATION Heavy Metal Atherosclerosis Antioxidant Metal Toxicity Free Radical Cleansing Lead Mercury Calcium Iron Cadmium Aluminum Copper Tin
Lead • 1. There is no safe level of lead in the body. • Environmental Health Perspectives, November 2007 • 2. Average person has 1000x the amount of lead in their • bodies than 400 years ago. • NEJM, April 1979 • 3. People with elevated lead levels have a 46% increased • all cause mortality, 39% increased mortality from circulatory disorders and 68% increased cancer • mortality. Concluded “no safe level of lead in body.” • Archives of Internal Medicine, November 2002
Lead • CDC ranks heavy metals as the number one environmental health threat for children. • Even low levels impair IQ. • NEJM, April 2003 • Release of lead from bones causes high blood pressure. Over 2000 women aged 40-59. • JAMA, 2003
Lead • Lead causes chronic renal failure and chelation therapy improves it. • American Journal of Medicine, August 2006 • Elevated blood lead levels increase the risk of strokes (151%) and heart attacks (89%). Circulation, October 2006
Lead • Lead affects the health of our brain- elevated bone levels cause 300% increased risk of • cataract. • JAMA, December 2004 • Lead makes mercury 100 times more toxic. • Toxicology and Environmental Health, 1978
Lead • Cumulative exposure to lead even at low levels may depress cardiac conduction. • Am J Cardiol 1988;82(5):594-599.
Lead • NHANES (National Health and Nutrition Examination Survey). • 2125 people over 40 • All lead levels were below “safe”level, but: • Higher the level>incidence arterial disease. • Highest quarter had 250% greater risk • Higher the level, higher the risk of death from heart attack over the next 16 years.
Mercury • Heart muscle of patients with idiopathic cardiomyopathy has 22000x the levels of mercury as normal heart muscle. • J Am Coll Cardiol 1999;33(6)
Chronic inflammation Chronic systemic inflammation is an underlying cause of many seemingly unrelated, age-related diseases. As humans grow older, systemic inflmmation can inflict devastating degenerative effects throughout the body (ward 1995; McCarty 1999; Brod 2000). This fact is often overlooked by the medical establishment, yet persuasive scientific evidence exists that correcting a chronic inflmmatory disorder will enable many of the infirmities of aging to be prevented or reversed.
Published Clinical Research All positive — No negative data All published studies are positive and show benefit • Many important studies were refused indexing by MEDLINE computerized index (censorship) • Five indexed studies with positive data showing benefit were published with deceptive negative conclusions: 1. Kitchell et al 1963, American Heart Journal, Reappraisal 2. Sloth-Nielsen, Guldager, et al 1991 Danish Study 3. Can Rij, et al 1994 New Zealand Study 4. Knutson, Andersen, et al Canada 2004, PATCH Study 5. Diehm, Schettler, et al 1986 Heidelberg StudyFor detailed analysis and scientific references: www.drcranton.com
Opinions on chelation therapy in patients undergoing coronary angiography: Cross-sectional survey Hude Quan, MD PhD. 1,2 P Diane Galbraith, MSc, 1,2 Colleen M Norris, PhD, 3Danielle A Southern, MSc, 1,2 Kathryn King, PhD, 1,2,4 Maria J Verhoef, PhD, 1 Merril L Knudtson, MD, 3 and William A Ghali, MD, MPH1,2,5 Can J Cardiol. 2007 June; 23(8) 635 - 640
Results Of the 780 patients who receive surveys. • 96 users and 264 nonusers of chelation therapy completed questionnaires. • Among the users, 20.8% believed that chelation therapy could cure heart disease, • 44.2% believed that it could relieve symptoms, • 16.7% believed that it could have side effects and • 58.4% believed that it could increase quality of life.
Results: (Continue) Users and nonusers were similar in their beliefs about safety and benefits of heart surgery, but users of chelation therapy were less likely than nonusers to believe that using conventional medications could prevent worsening of heart disease (53.1% vesus 67.4%), increase quality of life (74.0% versus 85.2%) and give a feeling of control over heart disease (61.5% versus 77.7%)
Chelation Therapy • 283 patients treated with EDTA for CVD over • 4 years • 87% improved • Clarke and Mosher, Am J Cardiol 1960;6:233
Chelation Therapy • EDTA decreased cancer incidence in 59 • patients over 18 years by 90%. • Only 1 of the 59 (1.7%) died of cancer • compared to 17.6% in non-treated, • matched subjects. • Blumer and Reich, Env Int 1980
Chelation Therapy • 2870 patients treated with EDTA • 77% CAD patients better • 91% PVD patients markedly better • Olszewer and Carter, Med Hypoth 1988;27:41-49
Chelation Therapy • 58 of 65 cancelled CABG. • 24 of 27 cancelled amputation. • J Adv Med 1993
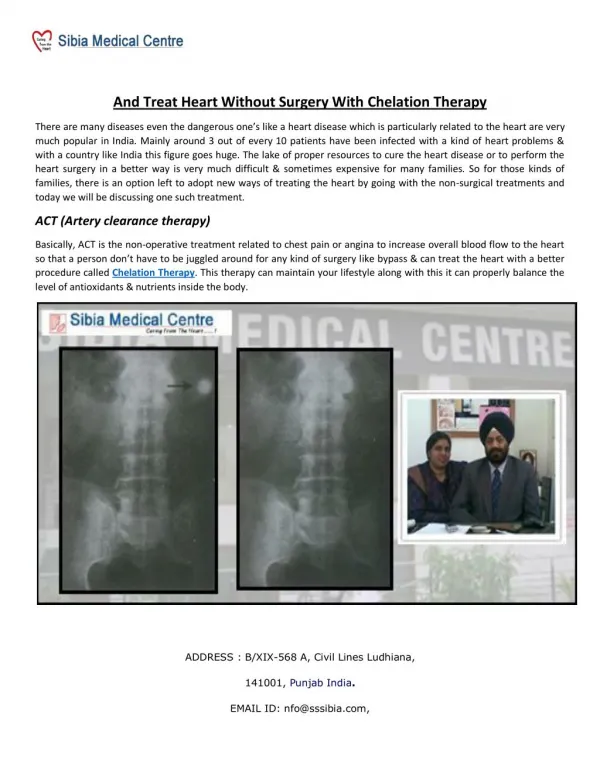
Prof. K H Yeoh EDTA ChelationClinical Photos Male, 67 yrs. IHD, Hypertension, Diabetes, Balloon Angioplasty Mar 2000 – Advised below knee amputation. EDTA commenced July 12, 2000
Prof. K H Yeoh EDTA ChelationClinical Photos April 20, 2001
Chelation Therapy • Marked improvement in 76/80 patients treated with EDTA for PVD. • Escobar, Surgery and Surgeons 1995.
Chappell Meta Meta-Analysis 1 • 19 studies on chelation therapy in CVD. • 22765 patients. • 87% favourable outcome. • J Adv Med 1993;6(3):139-160
Chappell Meta Meta-Analysis 2 • Retrospective analysis of 8 US chelation clinics. • Proven coronary artery disease. • Had at least 20 chelations. • 3 year follow up. • 248 patients. • Control group- CABG/stents.
Auckland Chelation Unit Data • 1500 consecutive patients. • No severe reactions. • Angina patients: • 5% greatly improved • 48% much improved • 25% mildly improved
Chelation Therapy • Ankle/brachial Doppler blood pressure ratio increased from 55% to 71%. • Journal of Advancement in Medicine, 1989 • Significant improvement in blood flow to brain. • Journal of Advancement in Medicine, 1989
ChelationTherapy • Brazilian study of 2870patients with heart disease: • 77% marked improvement • 17% good improvement • 4% partial improvement • 3% unchanged • Journal of Advancement in medicine, 1989
The Vulnerable Plaque • 85% of Myoardial Infarctions are not from progressive stenosis of the vessel • Vaso-spasm from increased free radicals and the vulnerable plaque account for this vast majority
The Vulnerable Plaque • vulnerable plaque may be buried inside the artery wall and may not always bulge out and block the blood flow through the artery
The Vulnerable Plaque • Fat droplets are absorbed by the artery – release of inflammatory cytokines • Arterial wall become sticky – attracts by monocyte • Monocyte squeeze into the arterial wall and turn to macrophage and begin to soak up fat droplets – foam cell • The fat-filled cells form a plaque with a thin covering.
The Vulnerable Plaque • The Oxidized lipids from the lipid core burst through the fibrous cap • These lipids crave electrons and get them from the blood products – sometime causing a complete thrombosis and infarct
The Vulnerable Plaque Several autopsy studies have demonstrated that nearly 70% of coronary thrombi occur at sites where the fibrous cap covering an atheromatous plaque has ruptured. Davies MJ, Thomas A. Thrombosis and acute coronary-artery lesions in sudden cardiac ischemic death. N Engl J Med. 1984; 310:1137–1140. Falk E. Plaque rupture with severe pre-existing stenosis precipitating coronary thrombosis. Characteristics of coronary atherosclerotic plaques underlying fatal occlusive thrombi. Br Heart J. 1983;50:127–134.
การได้รับสัมผัส • บุคคลที่มีอาชีพและงานที่เสี่ยงต่อการได้รับพิษสารหนู – เกษตรกร – อุตสาหกรรมแก้ว – ประชาชนทั่วไป • การเข้าสู่ร่างกายของสารหนู – การกินอาหารน้ำยารวมไปถึงสิ่งที่ปนเปื้อนสารหนู การหายใจเอาฝุ่นสารหนูเข้าไปและการดูดซึมทางผิวหนัง • พบได้ทั่วไปในดิน น้ำ อากาศ ทั้งสารประกอบอินทรีย์(organic arsenic) และสารประกอบอนินทรีย์(inorganic arsenic)
Table 2. Number of DM patients and rate of DM per 100,000 people in Nakhon Si Thammarat Province from 2003 – 2008 (Data from provincial health office) • Data as of 2003, ** use Nakhon Si Thammarat provincial data which is different from the • annual epidemiological surveillance report of the epidemiological division.
การได้รับสัมผัส บุคคลที่มีอาชีพและงานที่เสี่ยงต่อการได้รับพิษตะกั่ว • ผู้ที่ทำงานในเหมืองแร่และโรงงานถลุงแร่ตะกั่วผู้ที่ทำงานในโรงงานอุตสาหกรรมที่ใช้ตะกั่วเป็นองค์ประกอบ • ตำรวจจราจร การเข้าสู่ร่างกายของตะกั่ว • การกินอาหารน้ำยารวมไปถึงสิ่งที่ปนเปื้อนตะกั่วการหายใจเอาฝุ่นตะกั่วเข้าไปและการดูดซึมทางผิวหนัง
พิษจลนศาสตร์ของตะกั่ว(Toxicokinetics)พิษจลนศาสตร์ของตะกั่ว(Toxicokinetics) • ตะกั่วจะทำลายทั้งระบบประสาทส่วนกลางและระบบประสาทส่วนปลายยิ่งอายุน้อยระบบประสาทยิ่งถูกทำลายมาก • มีความสัมพันธ์ระหว่างการได้รับตะกั่วกับความอ่อนแอในความตั้งใจ ต่อต้านสังคมหรือพฤติกรรม เนื่องจากผลกระทบจากการพัฒนาระบบประสาท