Download

1 / 65
660 likes | 1.23k Views
Chelation Therapy and Hyperbaric Oxygen Therapy (HBOT). Presented by Tim Flanagan Caldwell College. Definitions.

E N D
Chelation Therapy and Hyperbaric Oxygen Therapy (HBOT) Presented by Tim Flanagan Caldwell College
Definitions • Complementary and alternative medicine (CAM) is defined by the National Center for Complementary and Alternative Medicine as “a group of diverse medical and health care systems, practices, and products that are not presently considered to be part of conventional medicine.” • An alternative definition offered by the Cochrane Collaboration is “a broad domain of healing resources that encompasses all health systems, modalities, and practices and their accompanying theories and beliefs, other than those intrinsic to the politically dominant health systems of a particular society or culture in a given historical period.” Myers & Johnson, 2007
How Widespread is the Use? • Almost one third of the children already had received a complementary or alternative therapy by the time they received a formal diagnostic evaluation for a suspected ASD • One survey in a private-practice population found that 92% of parents who responded had used CAM therapies for their children with ASDs • Another parent survey found that 52% of the children with an ASD had been treated with at least 1 CAM therapy, compared with 28% of a group of control children without disabilities • Surveys indicate that only 36% to 62% of caregivers who used CAM therapies for their children with ASDs had informed the child’s primary care physician Levy, Mandell, & Herhar (2003); Levy and Hyman (2008); Myers & Johnson, (2007)
Complementary and Alternative Medical Therapies (CAMs) Carr & LeBlanc (2007); Levy & Hyman (2005)
Hyperbaric Oxygen Therapy (HBOT) • Autism and HBOT Hyperbaric Chambers
Search Terms • PsychInfo • “HBOT” + “autism” • “Hyperbaric Oxygen” + “autism” • “Hyperbaric Oxygen Therapy” + “autism” • All of the above with “ASD”, “autism spectrum disorder” • Google Search • All of the above terms • Identified six articles • Reference Sections of Identified Articles
HBOT • The cost of treatment may range up to $150 per hour • Families report using anywhere from 40 to 120 h of HBOT • These hours are in lieu of other therapies such as applied behavior analysis, speech therapy, and occupational therapy and do not include travel time to the medical center where the therapy is provided • A number of websites focus on renting ($1,395 per month) and selling($8,495–27,995) chambers to families • Autism is not approved as an indication for HBO2 therapy • Undersea and Hyperbaric Medical Society • European Committee for Hyperbaric Medicine Levy & Hyman (2008); Yildiz, Aktas, & Uzun (2008)
Rationale • The mechanism of action of hyperbaric treatment in autism is not entirely known • Possibilities include: • Diminishing gastrointestinal and cerebral inflammation • Improving cerebral hypoperfusion • Decreased blood flow through the brain • Especially of the temporal lobes, reportedly affecting up to 75% of individuals with autism • Modulating immune dysregulation Rossignol & Rossignol (2006); Rossignol (2007)
Rationale • HBOT has been used with other populations where cerebral hypoperfusion is expected • Cerebral palsy, fetal alcohol syndrome, closed head injury, and stroke • HBOT can compensate for decreased blood flow • Increasing the oxygen content of plasma and body tissues • Normalize oxygen levels in ischemic tissue • Animal studies have shown that HBOT has anti-inflammatory effects and reduces oxidative stress • Up-regulation of antioxidant enzymes • Can help with detoxification problems specifically found in autistic children • HBOT may mobilize stem cells from human bone marrow, which may aid recovery in neurodegenerative diseases • Stem cells can enter the brain and form new neurons, astrocytes, and microglia Rossignol & Rossignol (2006); Rossignol (2007)
Additional Claims • HBOT can increase the function and production of mitochondria and improve neurotransmitter abnormalities • Some children with autism have dysfunctional mitochondria, the energy generating parts of the cell • Animal studies have demonstrated increased mitochondrial efficiency and mitochondria density with HBOT • HBOT can improve this dysbiosis which is common in autistic children • Refers to a condition with microbial imbalances on or within the body (e.g., “leaky gut”) • HBOT might help overcome the effects of the impaired production of porphyrin Rossignol (2007); Van Dyke (2009)
To Summarize • Autism is a neurodegenerative disease characterized by • Cerebral hypoperfusion • Neuro-inflammation • Increased oxidative stress • HBOT • Helps overcome hypoperfusion • Has potent anti-inflammatory effects • Reduces oxidative stress • Mobilizes stems cells from human bone marrow • Therefore, HBOT will improve symptoms of autism Rossignol & Rossignol (2006)
Potential Side Effects • Hyperbaric treatment for children is generally regarded as safe, even at pressures of 2.0 atm and 100% oxygen for two hours per day • Most common side effects • Barotrauma (2% incidence) • Discomfort and possible damage in the ear due to pressure differences between the inside and outside of the eardrum • Sinus squeeze • Serous otitis • Claustrophobia • Reversible myopia • New onset seizure (which occurs in 1–3 per 10,000 treatments) Levy & Hyman (2008); Rossignol & Rossignol (2006); Rossignol (2007); Rossignol (2009)
History • Heuser, G., Heuser, S.A., Rodelander, D., Aguilera, O., Uszler, M. (2002) treated a four year old autistic child using lower pressure HBOT at 1.3 ATA • Reported ‘‘striking improvement in behavior including memory and cognitive functions’’ • Improvement of cerebral hypoperfusion as measured by pre-HBOT and post-HBOT SPECT scans Rossignol (2009)
History • This treatment has increased in recent years and traditionally involves inhaling 20-100% oxygen at a pressure greater than one atmosphere (atm) in a pressurized chamber • The pressure provided by the HBOT chamber (typically 1.3 to 1.5 absolute atmospheres [ATA]) promotes the dissolution of oxygen into the blood. The oxygen is then circulated near dormant or injured tissue in the body • Two case reports and three uncontrolled studies enrolling between 6 and 18 children with autism have reported clinical improvements with hyperbaric treatment at 1.3 atm • One study treated children with autism with the use of hyperbaric treatment at both 1.5 atm/100% oxygen and 1.3 atm/24% oxygen; • Neither hyperbaric protocol worsened markers of oxidative stress and both reduced C-reactive protein (a marker of inflammation) Levy & Hyman (2008); Rossignol (2009); Schechtman (2007)
History • In their review of the literature at the time, Levy and Hyman (2008) graded the use of HBOT for individuals with autism as a C (based solely on case reports or theories) • “The subjective data and potential confounds make this study difficult to interpret. There are no randomized controlled trials of HBOT for symptoms of ASD to support the clinical use of this modality” • Similarly, Lerman et al. (2008) stated, “the neurological abnormalities referenced have not been verified and no controlled studies have been conducted on the behavioral outcomes of HBOT with this population” Lerman et al. (2008); Levy & Hyman (2008)
Evidence • First controlled trial reported in 2009 • 66 children, 2 to 7 years of age • Diagnosis of Autistic Disorder • No previous hyperbaric treatment • DSM-IV criteria for Autistic Disorder • Diagnosis corroborated • Autism Diagnostic Interview–Revised (ADI-R) • Autism Diagnostic Observation Schedule (ADOS). • Exclusion criteria • PDD-NOS, Asperger syndrome, seizure disorder, current ear infection, uncontrolled asthma, inability to equalize ear pressure, fragile X syndrome, and ongoing treatment with chelation medication Rossignol et al. (2009)
Design • Treatment group • 1.3 atm and 24% oxygen for 40 sessions lasting 1 hour each • Control group • Slightly pressurized room air at 1.03 atm and 21% oxygen for 40 sessions lasting 1 hour each • Identical number of treatments (40 sessions) and overall treatment period (4 weeks) • Twice a day separated by a minimum of 4 hours, 5 days per week, for 4 consecutive weeks, for a total of 40 treatments per child. Rossignol et al. (2009)
Outcome Measures • Aberrant Behavior Checklist–Community (ABC) • Parent or primary caretaker • Autism Treatment Evaluation Checklist (ATEC) • Parent or primary caretaker • Clinical Global Impression– Improvement (CGI) • Parent or primary caretaker • Rated separately by the treating physician (without knowledge of the parental ratings) Rossignol et al. (2009)
Results • Statistically significant improvements • Overall functioning, receptive language, social interaction, eye contact, and sensory/cognitive awareness • Children who were over age 5 had significantly better improvements on the ABC total score • Children who had lower initial autism severity also had the most improvements • Comparison of pre- and post-ADOS performed by blinded assessors demonstrated no significant change in autism diagnosis between the two groups Rossignol et al. (2009)
Results • 80% of children in the treatment group had an improvement on the CGI physician scale for change in overall functioning • 38% of children in the control group were also rated as improved • Improvements observed in the control group could have been due to the slight hyperbaric pressure received • 73% of parents of children in the control group rated their child as improved on the CGI scale Rossignol et al. (2009)
Criticism of the Study • The ATEC has not been validated • Inclusion in a study such as this questionable. • The authors reported a significant difference between groups on both the physician CGI and the parent CGI • No baseline measure was completed by the physicians prohibiting the authors from detecting a pre-post effect based on their ratings • Physicians failed to complete the entire CGI • Focused on one item. Jepson et al (2011)
Evidence • 3 children with autism who had been receiving intensive behavioral intervention for 8 months to 4.5 years • HBOT sessions took place in a chamber that provided the participants with 88% (+/- 3%) oxygen at 1.3 ATA (according to the manufacturer) and is sold for in-home use • Forty 60-min sessions in a hyperbaric oxygen chamber • Child was gradually acclimated to the oxygen mask and the chamber • Participants were videotaped three times each week during structured, 10-min instructional sessions • These sessions were conducted before the HBOT intervention began and continued throughout the intervention period. For all children, sessions continued for an additional month after the HBOT sessions ended • Separation of at least 2 hours between the HBOT and instructional session • The observers were unaware of the purpose of the study, the intervention evaluated, or the point at which the intervention was introduced Lerman et al. (2008)
Design • Concurrent multiple-baseline across participants • Baseline phase for each successive participant lasted a minimum of 20 days longer than that for the previous participant • Child had continuous access to preferred items (e.g., portable DVD players, puzzles, books) while in the HBOT. • Relative to baseline, the introduction of HBOT was necessarily associated with a 60-min daily reduction in instruction at the center, along with an increase in access to preferred activities
Dependent Measures • Specific responses related to task engagement, language, and problem behavior were defined for each participant • Behavior of the therapist also measured. • Delivery of verbal instructions • Delivery of praise • Delivery of tangibles Lerman et al. (2008)
Procedures • A representative sample of targets from the child’s current curriculum was selected for use during the instructional sessions • Sessions included only those acquisition targets that were currently completed with 50% accuracy or less, on average • An acquisition target was removed from the sessions when the child’s accuracy on the target during regular educational therapy sessions exceeded 50% correct for three consecutive days • A new target from the same skill domain but for which current performance did not exceed 50% accuracy replaced the previous target Lerman et al. (2008)
Procedures • 12 to 15 different acquisition targets were included in each session interspersed with mastered targets • A maintenance target was presented after three consecutive presentations of acquisition targets. • Instructional trials were delivered every 30 s • IOA was measured during 25% of the sessions • 2 of 3 children experienced a total of 40 “dives” • Third child was withdrawn after 27 “dives” • Eye infection unrelated to HBOT Lerman et al. (2008)
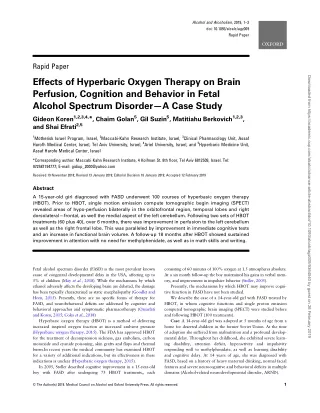
Figure 1. Percentage of task engagement across baseline, HBOT, and post-HBOT conditions for Lillie, Carl, and Harvey. Calendar dates appear below the session numbers.
Results • HBOT was not associated with any obvious changes in the level, stability, or trend of task engagement compared to baseline for the three children • A somewhat abrupt increase in task engagement coincided with the removal of HBOT • Therapist began to deliver more prompts to attend to the task materials during this phase • M = .37 rpm during HBOT; M= .74 rpm following HBOT Lerman et al. (2008)
Figure 2. Responses per minute of problem behavior across baseline, HBOT, and post-HBOT conditions for Lillie, Carl, and Harvey. Calendar dates appear below the session numbers.
Results • Overall results do not suggest that HBOT enhanced the effects of ongoing behavioral intervention • Slight increase in problem behavior for Carl with the removal of HBOT • Confounding component of the HBOT? • Spending an hour each day with preferred activities Lerman et al. (2008)
Figure 3. Responses per minute of spontaneous communication across baseline, HBOT, and post-HBOT conditions for Lillie, Carl, and Harvey. Calendar dates appear below the session numbers.
Results • The introduction of HBOT for Harvey appeared to be associated with an increase in spontaneous communication • Similar levels persisted for up to a month after HBOT was terminated • It is possible that HBOT produced idiosyncratic outcomes across the participants, with positive effects obtained for Harvey only • Alternatively, the increase in Harvey’s spontaneous communication may have been the result of • Ongoing behavior analytic intervention, or • Changes in an unknown variable that occurred simultaneously with the introduction of HBOT Lerman et al. (2008)
Potential Confounds • Reduction in instruction (by 60min per day) • Access to preferred activities • Procedural drift Lerman et al. (2008)
Evidence • Granpeesheh et al. (2010) conducted a randomized, double-blind, placebo controlled evaluation of HBOT • 80 1-h sessions at 24% oxygen and 1.3 ATA • Administered 6–10 times per week • 18 participants in the treatment group and 16 controls • Both groups improved to a small degree • No significant difference in improvement between groups • All participants were also receiving behavioral intervention services Granpeesheh et al. (2010)
Evidence • Jepson et al. (2011) evaluated the effects of HBOT on direct measures of 11 topographies of behavior • Five replications of multiple baselines across children • Total of 16 participants • Inclusion criteria were as follows: • Diagnosis of autistic disorder, pervasive developmental disorder not otherwise specified (PDD NOS), or Asperger’s disorder • Between 2 and 10 years of age • No change in medical treatment regimen or dietary regimen for 6 weeks prior to the study • Agreement to refrain from changing any treatment regimens during the course of the study • Potential participants were excluded if they displayed any medical conditions which would contraindicate HBOT (e.g., current otitis media, current sinus infection, history of seizures)
Dependent Measures • Frequency data were collected on: • (a) vocal initiations • (b) physical initiations • (c) vocal response to a therapist vocalization (e.g., saying ‘‘thank you’’ in response to a compliment) • (d) physical response to a therapist behavior (e.g., showing a toy air plane in response to a therapist saying ‘‘Look, I have a cool car’’) • (e) self-injurious behavior or aggression • (f) disruption • (g) tantrums • (h) vocal stereotypy • (i) physical stereotypy • Ten-second partial interval data were collected on: • (a) toy contact • (b) physical activity Jepson et al. (2011)
Design • Non-concurrent multiple-baseline across participants • Four non-concurrent multiple baselines were conducted across three participants • One non-concurrent multiple baseline was conducted across four participants Jepson et al. (2011)
Procedures • Behavioral observation play sessions were 10 min • Twice per week during the baseline phase, immediately prior to each HBOT session, and at all follow-up appointments • Research assistants were not informed of the purpose of the study • However, participants received HBOT therapy immediately after the play session. • (IOA) was assessed for at least 32% of all sessions for each participant Jepson et al. (2011)
Procedures • 24% oxygen at 1.3 ATA • Each participant received a total of 40 HBOT sessions over an average of 56 days (r = 39–68). • Two follow-up direct observation play sessions 2 weeks after the last HBOT session and for two additional direct observation play sessions 3 months after the last HBOT session. • Graphic displays for each topography of each participant not provided due to space limitations • Data for individual participants were summed three in classes: • Adaptive behavior • Stereotypy • Aberrant behavior Jepson et al. (2011)
Results • A visual inspection of changes in level, trend, and variability reveal no consistent effect on any class of behavior across any of the multiple baselines • No clear effect was apparent for any individual participant • Rossignol et al. (2009) used almost twice the average number of treatment sessions per week • Did not replicate the positive findings demonstrated in one of the participants in the (Lerman et al. 2008) study • Increases the probability that the effect seen in the Lerman participant was an aberration Jepson et al. (2011)
Limitations • Did not require participants to actively engage in a learning task or memory activity • Measures of possible changes in biochemical variables were not collected (e.g., markers of inflammation or oxidative stress) • Participants were not included or excluded based on their physical well-being • Possible that those with more physical dysfunction may have responded as a group Jepson et al. (2011)
Summary • What conclusions can be drawn? • Questions? Comments?
Chelation Therapy • Jim Adams, Autism & Chelation on Dateline NBC pt 1 • Jim Adams, Autism & Chelation on Dateline NBC pt 2
Search Terms • PsychInfo • “Chelation” + “autism” • “Chelation Therapy” + “autism” • “Chelation Treatment” + “autism” • All of the above with “ASD”, “autism spectrum disorder” • Google Search • All of the above terms • Identified 13 studies • All but one were correlational studies, reviews or critiques, surveys, or responses to one of the above • Reference Sections of Identified Articles
Yes, You’ve Heard This Before • Up to five of the patients in Wakefield’s original study were involved in a lawsuit against vaccine manufacturers prior to their participation in the study • Wakefield received up to 55,000 British pounds to assist their case by finding evidence linking autism with the MMR vaccine • In March of 2004, ten of the original authors issued a retraction of the “interpretation of their findings” • They subsequently agreed to “…formally retract the interpretation placed upon the findings in this paper…” Doja & Roberts (2006)
Rationale • Chelation is a detoxification process to remove heavy metals from the bloodstreams of individuals who have suffered metal poisoning by administering either DMPS (2,3-dimercaptopropane-1-sulfonate) or DMSA (2,3-dimercaptosuccinic acid) • These agents bind heavy metals such as mercury and facilitate elimination from the body • It was first introduced to populations with autism in response to the theory that autism is caused by elevated levels of mercury and other heavy metals in the body • Chelation can occur through ingestion of pills, through creams, or intravenously Doja & Roberts (2006); Levy & Hyman (2005) Levy & Hyman (2008); Weiss, Fiske, & Ferraioli (2008)
Rationale • Certain individuals may exhibit severe adverse reactions to low doses of mercury, which are otherwise largely benign to the majority of those exposed • Because glutathione has a role in eliminating toxic substances from the body, a deficiency could cause autistic children to have predisposition to ethylmecury toxicity from thimerosal • Some strains of mice have enhanced genetic susceptibility to the effects of mercury • By extension, some children may also have enhanced genetic susceptibility Bernard et al. (2002); Doja & Roberts (2006); Levy & Hyman (2005)
Rationale • Symptoms of mercury toxicity can arise suddenly in especially sensitive or sensitized individuals, but expression is usually gradual • Autistic symptoms usually emerge gradually although there are instances of sudden onset • Nearly all American children are immunized but few have ASD • This pattern is consistent with response to low dose mercury exposure, which is characterized by wide individual variation Bernard et al. (2002)
Rationale • Because autism likely involves a broad range of genetic, prenatal, social, developmental, nutritional, and environmental factors, and it is unlikely that only one treatment will be effective • Autistic children often have lower levels of detoxification enzymes and antioxidants and may therefore be more susceptible to environmental toxics • Autistic children have significantly lower mean levels of detoxification/antioxidant enzymes such as paroxonase, sulphation enzymes, glutathione peroxidase,and superoxide dismutase Curtis & Patel (2008)
Criticism of the Rationale • Since 2001, thimerosal present in amounts large enough to act as a preservative have been removed from all childhood vaccines except for a few influenza and hepatitis vaccines • In Canada, the most common childhood vaccines have been free from thimerosal since 1992 • Methylmercury is transported across the blood-brain barrier via an active transport system, whereas ethyl mercury is not. • Methylmercury is far more likely to cause nervous system toxicity. • A series of subsequent studies all found no link between thimerosal and autism Doja & Roberts (2006)