Download
1 / 1
10 likes | 314 Views

E N D
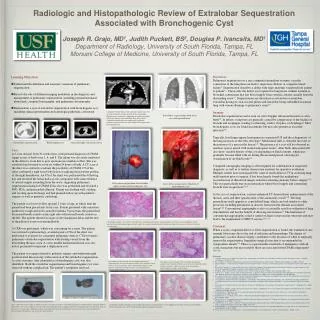
Radiologic and Histopathologic Review of Extralobar Sequestration Associated with Bronchogenic CystJoseph R. Grajo, MD1, Judith Puckett, BS2, Douglas P. Ivancsits, MD1Department of Radiology, University of South Florida, Tampa, FLMorsani College of Medicine, University of South Florida, Tampa, FL Discussion: Pulmonary sequestration is a rare congenital anomalous systemic vascular connection of the lung than can lead to respiratory distress or congestive heart failure1. Sequestration describes a defect with large anatomic variation from patient to patient1,2. Classically, the defect is recognized as lung tissue without tracheal or bronchial connections that has blood supply from systemic arteries, usually from the descending aorta1,3. Sequestrations are described as extralobar or intralobar, extralobar having its own visceral pleura and intralobar being embedded in normal lung with venous drainage to pulmonary veins2,3. Imaging: Extralobar sequestration can be seen on color Doppler ultrasound in utero or after birth4,5. In infants, symptoms are generally caused by compression of the trachea or bronchi and esophagus, leading to wheezing, stridor, dyspnea, or dysphagia4. Most bronchogenic cysts are found incidentally but may also present as recurrent infection4,6. Typically, fetal lungs appear homogeneous on prenatal US and the echogenicity of the lung increases as the fetus develops4. Mediastinal shift is often the first clue to the presence of a mass in the thorax3,4. The presence of a cyst will be observed as anechoic spaces mixed with normal echogenic tissue5. After birth, ultrasound will also show variable density of the cyst depending on fluid contents ,which may gradually become filled with air during the neonatal period, allowing for visualization of air-fluid levels4,5. Computed tomography imaging is often required for confirmation of suspected diagnosis, as well as to further characterize anatomy for operative evaluation. Multiple studies have investigated the value of multi-detector CT in assessing lung malformation prior to surgery. It has been largely found that multiplanar reconstruction of thin sliced images aided in evaluating anatomy before surgery4,7,8. This was particularly true in circumstances where blood supply and connecting bronchi were in question4,7,8,9. In the case of sequestration, contrast-enhanced CT demonstrates enhancement of the thoracic aorta and then opacification of the anomalous vessel3,10. The lung parenchyma itself appears as consolidated lung, which can look similar to other processes including pneumonia or abscess formation but remains an isolated lesion3,10. Conventional angiography is also occasionally used for evaluation of lung abnormalities and has the benefit of allowing intervention13. The limitation of conventional angiography is that it cannot evaluate extravascular structures and may lead to the requirement of MDCT anyway11,12,13. Treatment: When a cystic congenital defect or lobar sequestration is found, the standard of care remains lobectomy due to the risk of infection and hemorrhage. The degree of pulmonary vascular disease largely contributes to the decision of when to surgically remove the sequestration. Immediate surgical resection is recommended in symptomatic infants1,4. There is a questionable small risk of malignancy with all cystic formations but most notably those are associated with CPAM components1, 14,15,16. • Learning Objectives • Understand the definition and anatomic variations of pulmonary sequestration • Review the role of different imaging modalities in the diagnosis and management of pulmonary sequestration, including prenatal/antenatal ultrasound, computed tomography, and pulmonary arteriography • Demonstrate a case of extralobar sequestration with bronchogenic cyst, including clinical presentation and radiologic/pathologic correlation Case: A 2-year old girl, born 39-weeks term, with prenatal diagnosis of CPAM. Apgar scores at birth were 1, 6, and 8. The infant was electively intubated in the delivery room due to poor spontaneous ventilator effort. She was extubated and weaned to room air within 24 hours of birth. A CT scan of the chest was ordered to evaluate the possibility of CPAM. CT of the chest confirmed a right lower lobe lesion occupying the posterior portion of the right hemithorax. An US of the chest was performed the following day and revealed the lesion had a cystic component with some evidence of arterial supply extending from the aorta, suggesting pulmonary sequestration instead of CPAM. Echo also was performed and revealed a PFO, PDA, and pericardial effusion. Patient was feeding well, voiding and stooling upon discharge and had planned follow up with pediatric surgery as well as pediatric cardiology. The patient was lost to follow up until 2 years of age, at which time the patient had been placed into foster care. Patient presented with consistent productive cough and well-controlled asthma. Upon exam, the patient had decreased breath sounds on the right side with normal breath sounds on the left. The patient showed no signs of developmental delay and the rest of the physical exam was unremarkable. A CXR was performed, which was concerning for a mass. The patient was referred to pulmonology, at which point a CTA of the chest was performed to evaluate for congenital pulmonary defects. CTA revealed a pulmonary extralobar sequestration with feeding vessels from the descending thoracic aorta. A cystic middle mediastinal lesion was also noted, presumed to represent a duplication cyst. The patient was again referred to pediatric surgery and underwent right posterolateral throacotomy with resection of the extralobar sequestration. A cystic structure, later identified as a bronchogenic cyst, was also identified. Both the extralobar sequestration and bronchogenic cyst were removed without complication. The patient’s symptoms resolved. Coronal CT of the thorax with contrast demonstrates two arterial structures arising directly off the descending thoracic aorta (red arrow) supplying the right paraspinal soft tissue density at the right lung base (blue circle). Additional round right paraesophageal hypodense structure (green arrow) was later confirmed to represent a bronchogenic cyst. Extralobar sequestration with focal area of hyperinflation Extralobar sequestration Bronchogenic cyst Aberrant right subclavian artery Gross intra-op specimen of extralobar sequestration and bronchogenic cyst Gross intra-op specimen of ligation of bronchogenic cyst Histologic section (2x and 4x) through the extralobar pulmonary sequestration near the vascular pedicle, which demonstrates disordered parenchyma with changes of bronchectasia (yellow arrow) and areas of mucin retention (red arrows). References: Thilenius, Otto G., et al. "Spectrum of pulmonary sequestration: association with anomalous pulmonary venous drainage in infants." Pediatric cardiology 4.2 (1983): 97-103. Bush, Andrew. "Congenital lung disease: a plea for clear thinking and clear nomenclature." Pediatric pulmonology 32.4 (2001): 328-337. Siegel, Marilyn J. "CT Evaluation of Pediatric Chest in Routine Practice." Diseases of the Heart and Chest, Including Breast 2011–2014 (2011): 39-46. Byyam DR, Chapman T, Ferguson MR, Deutsch G, Dighe MK. Congenital Lung Abnormalities: Embryologic Features, Prenatal Diagnosis, and Postnatal Radiologic-PathologicCorrelation. RadioGraphics (2010) 30:1721–1738. Enriquez, Goya, Celestino Aso, and Xavier Serres. "Chest ultrasound (US)." Pediatric Chest Imaging (2008): 1-35. Achiron, R., J. Hegesh, and S. Yagel. "Fetal lung lesions: a spectrum of disease. New classification based on pathogenesis, two‐dimensional and color Doppler ultrasound." Ultrasound in Obstetrics & Gynecology 24.2 (2004): 107-114. EGPLANNED= GOOD IMAGING El-medany, Sameh, et al. "Role of multi slice computed tomography in the evaluation of congenital anomalies of tracheobronchial tree and lungs." The Egyptian Journal of Radiology and Nuclear Medicine (2011). Lee, Edward Y., Phillip M. Boiselle, and Robert C. Shamberger. "Multidetector computed tomography and 3-dimensional imaging: preoperative evaluation of thoracic vascular and tracheobronchial anomalies and abnormalities in pediatric patients." Journal of pediatric surgery 45.4 (2010): 811. Lee, Edward Y., Phillip M. Boiselle, and Robert H. Cleveland. "Multidetector CT Evaluation of Congenital Lung Anomalies1." Radiology 247.3 (2008): 632-648. Papaioannou, Georgia, Carolyn Young, and Catherine M. Owens. "Multidetector row CT for imaging the paediatric tracheobronchial tree." Pediatric radiology 37.6 (2007): 515-529. Siegel, Marilyn J. "Multiplanar and Three-dimensional Multi–Detector Row CT of Thoracic Vessels and Airways in the Pediatric Population1." Radiology 229.3 (2003): 641-650. Papaioannou, G., C. Young, and C. Owens. "Volumetric Computed Tomography of the Tracheobronchial Tree." Diseases of the Heart, Chest & Breast (2007): 36-47. Konen, Eli, et al. "Congenital Pulmonary Venolobar Syndrome: Spectrum of Helical CT Findings with Emphasis on Computerized Reformatting1." Radiographics 23.5 (2003): 1175-1184. Loachimescu, O. C., and A. C. Mehta. "From cystic pulmonary airway malformation, to bronchioloalveolar carcinoma and adenocarcinoma of the lung." European Respiratory Journal 26.6 (2005): 1181-1187. Dishop, Megan K., and Supriya Kuruvilla. "Primary and metastatic lung tumors in the pediatric population: a review and 25-year experience at a large children's hospital." (2009). Priest, John R., et al. "Pulmonary cysts in early childhood and the risk of malignancy." Pediatric pulmonology 44.1 (2009): 14-30. Histologic section through the extralobar pulmonary sequestration near the vascular pedicle (10x) demonstrating areas of mucin retention within disordered alveoli (yellow arrows) and areas of inflammation surrounding these airways (red arrows). Histologic section through the extralobar pulmonary sequestration demonstrating areas of mucin retention within irregular airways (yellow arrows) and surrounding inflammatory changes (red arrows). Gross specimen of an irregular piece of lung tissue representing an extralobar pulmonary sequestration. Vascular pedicle (red circle) seen at the edge of the specimen corresponding to the supplying arteries originating from the thoracic aorta as seen on CT examination. Additional areas of purple-gray pleural lining (yellow arrows) and areas of dark brownish hemorrhagic components are also seen (blue arrows). Histologic section through the extralobar pulmonary sequestration at the opposite end from the vascular pedicle demonstrating areas of marked lymphangiectasia (green arrows).