Download
1 / 62
620 likes | 837 Views
PUTTING LYME BEHIND YOU Basic Lyme For Patients, Family And Friends. Joseph J. Burrascano Jr. M.D. March 2011. WHAT IS LYME DISEASE?. Lyme disease is the illness that results from the bite of an infected deer tick. TYPES OF LYME DISEASE. Early Lyme disease (“stage I”)

E N D
PUTTING LYME BEHIND YOUBasic Lyme For Patients, Family And Friends Joseph J. Burrascano Jr. M.D. March 2011
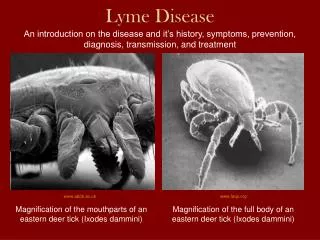
WHAT IS LYME DISEASE? Lyme disease is the illness that results from the bite of an infected deer tick .
TYPES OF LYME DISEASE • Early Lyme disease (“stage I”) • At or before the onset of symptoms • Can be cured if treated properly and promptly • Disseminated Lyme (“stage II”) • Multiple major body systems affected • More difficult to treat • Chronic Lyme disease (“stage III”) • Ill for one or more years- immune system breakdown and its consequences • Co-infections become important • Serologic tests less reliable • Treatment must be more aggressive and of longer duration .
DIAGNOSING LYME Lyme is a clinical diagnosis”- Why? • Only 17% recall a bite (Texas Dept. of Health; Dutchess Co. Dept. of Health) • Only 36% recall a rash (Texas Dept. of Health) • Only 50 to 70% have a positive ELISA or Western Blot Co-infections- their tests are even less sensitive .
WHAT ABOUT CO-INFECTIONS? • Ticks are “nature’s dirty needle”- may potentially contain hundreds of different types of germs, and these may be transmitted to you, along with classic Lyme, from the same tick bite • Nearly universal in chronic Lyme • Symptoms more vague, and overlap • Diagnostic tests LESS reliable • Co-infected patients more ill and more difficult to treat • Lyme treatments do not treat Babesia, Bartonella or viruses • One reason for “treatment-resistant” Lyme .
SORTING OUT CO-INFECTIONS • LYME- • Gradual onset of initial illness, no sweats, 4-week cycles • Multisystem, joint involvement, afternoon fevers • Bb antibodies usually present, low CD-57 • Herxheimer; otherwise, slow response to onset of antibiotics and slow relapse • BARTONELLA- • Gradual onset of initial illness, occasional light night sweats • More CNS symptoms than skeletal symptoms, with CNS irritability, GI upset, sore soles, subcutaneous nodules arms and legs, AM fevers, swollen lymph glands • Elevated VEGF • Rapid relapse of symptoms if treatment ended too soon or if treatment not optimal • BABESIA- • Abrupt onset of initial illness, obvious sweats especially at night, cycles every few days • Fatigue, global headaches, air hunger, cough, hypercoaguable (responds to Heparin) • Very severe Lyme symptoms and poor response of Lyme to otherwise appropriate treatment • EHRLICHIA- • Rapid onset of initial illness, may be high fevers and rarely spotted rash like RMSF • Headaches (knife-like and behind eyes), sore muscles • Low WBC, elevated liver function tests • MYCOPLASMA- • Gradual onset, may be light sweats, symptoms are made worse with exercise • Major fatigue and neurological dysfunction, metabolic disturbances, immune damage • Found in the sickest and poorest-responding Lyme patients (CFIDS-like, ALS) .
Lyme Disease Tests • Serologic tests (ELISA, western blots) miss 30% to 50% of cases • ELISAs are of little value (do Western Blots) • Can be 5% to 10% false positives • NOT an effective screening test! • Spinal tap- Only 9% have + CSF antibodies! • PCRs- 30 % sensitivity at best- requires multiple samples, multiple sources (whole blood, serum, urine, CSF, bone marrow, biopsy material) • LDA- Urine antigen capture (& reverse western blot)- similar sensitivity and specificity to PCR .
WHY IGENEX? • If a test is commercialized so it can be sold as a test kit to others, then it must follow narrow and restrictive CDC guidelines • These restrictions were a result of the Lyme vaccine debacle • The result is that all commercially available Lyme tests will miss up to 75% of cases!!!! • The only two labs with non-commercial tests are Igenex and Stony Brook (but Stony Brook will still follow CDC guidelines when reporting results) • In fact, based on blinded government proficiency tests, Igenex is the most accurate Lyme lab available in the USA and is licensed and accepted by Medicare and federal and all state governments. .
CD-57 COUNT(Natural Killer Cells) • Low counts seen in Chronic Lyme when the infection has been active > 1 year • Reflects degree of infection by Bb only, and not the co-infections • Can be a screening test for Bb infection • Does not change during treatment until Bb is controlled • Predicts a relapse if low when antibiotics end • Must be done by LabCorp’s methods (normal is >200) • <20- severe illness • 20-60- most common result in chronic patients • >60- Lyme activity minimal • >120- Relapse NOT likely after treatment ends .
CHRONIC LYME DISEASE-Why are patients so ill? • Higher spirochete load (multiple bites, infected longer) • Protective niches and biofilms- allow Bb to evade the immune system and antibiotics • Development of alternate forms of Bb • Immune suppression (co-infections become a bigger issue) and immune evasion • Many associated conditions occur as a result .
TREATMENT BACK TO BASICS! .
LYME TREATMENT Pharmacology • Critical to achieve therapeutic drug levels • Great variability patient to patient • Must measure peak and trough levels • Antibiotics must have extra- and intra-cellular sites of action • Bb can survive in both compartments • Not many antibiotics reach both places • Antibiotics must act in body fluids and in tissues • Bb lives in both compartments • Not many antibiotics do both .
LYME TREATMENT Alternate forms of Bb • SPIROCHETE FORM- has a cell wall • Penicillins, cephalosporins, Primaxin, vancomycin • L-FORM (spiroplast)- no cell wall • Tetracyclines, Erythromycins • CYST • Metronidazole, tinidazole • Rifampin? .
LYME TREATMENT Antibiotic Types Kinetics of killing B. burgdorferi • Cell wall agents and erythromycins • Need sustained bactericidal levels for 72 hours • Tetracyclines • Need a spike in blood level • Metronidazole • Sustained levels for two weeks! .
LYME TREATMENT Design of Regimen • ANTIBIOTIC COMBINATIONS- Must be designed to target: • Intracellular + extracellular sites • Body fluid + tissue compartments • The three known morphologic forms .
ANTIBIOTICS- ROUTE OF ADMINISTRATION Repeated Antibiotic Treatment in Chronic Lyme Disease (Fallon, JSTBD, 1999) • No response to placebo • Slight benefit from oral antibiotics • Intramuscular benzathine penicillin more effective than oral antibiotics • Intravenous therapy most effective .
INDICATIONS FOR INTRAVENOUS THERAPY • Illness for more than one year • Prior use of steroids • Documented immune deficiency • Abnormal spinal fluid (↑WBC,↑ Protein) • Synovitis with high ESR • Age over 60 • Acute disseminated illness in first trimester • Acute carditis • Failure or intolerance of oral therapy .
TYPICAL REGIMEN IN CHRONIC LYME • ORAL- • Cefuroxime + clarithromycin • Augmentin XR + telithromycin • INJECTION- • Bicillin LA + clarithromycin • INTRAVENOUS- • Ceftriaxone + telithromycin • Vancomycin + clarithromycin Tinidazole or metronidazole can be added to these .
CHRONIC LYME Treatment Issues-1 • In chronic Lyme Disease, infection may persist despite prior antibiotic therapy • Relapses do occur and retreatment is often needed • Repeated or prolonged antibiotic therapy usually is necessary • Aggressive supportive therapy is required .
CHRONIC LYME Treatment Issues-2 • High doses of antibiotics are needed, and blood levels should be confirmed • Antibiotic combinations usually necessary • Check for co-infections and immune status, and treat appropriately • May need to rotate through different regimens based on response .
CHRONIC LYME Treatment Issues-3 • Rate of recovery is a function of the biology of Borrelia, and a stronger drug will not speed up recovery! • Goal therefore is to find a regimen that is working, and stay on it long term • Change regimens only when reach a plateau with continued active symptoms • Do not change treatment every few weeks- give each regimen at least six weeks, and preferably three+ months before the regimen is changed! .
CHRONIC LYME Treatment Issues-4 • As symptoms wind down, I DO NOT cut the dose, for resistance may develop • Progressively increase exercise program as the symptoms of Lyme decrease • Exercise is vital and required, or a full recovery will not occur • Not exercising will increase risk of a relapse .
CHRONIC LYME Treatment Issues-5 • If the CD-57 count is not normal at the end of treatment, then continued illness or a relapse is likely • May not cure the infection, and may need open- ended maintenance therapy • Signs of persistence of infection: • continued fevers, synovitis • four week cycles, migrating symptoms • Positive PCR or urine LDA • low CD-57 counts .
BARTONELLA-LIKE ORGANISMS • More prevalent in some ticks than even Borrelia! • Clinically, seems to be a different species than “cat scratch disease” (?Tularemia) • CSD Tests are insensitive! (serologies and PCR) • Serologies miss up to 80% of clinically defined cases • New FISH test is now available from Igenex • Clinical clues: • CNS symptoms out of proportion to physical • Encephalopathy-encephalitis, irritability, anxiety, insomnia, seizures, gastritis, rashes, tender skin nodules, sore soles, AM fevers, light night sweats • Persistent CNS symptoms despite Lyme Rx • Specific rash .
Bartonella Rashes Red bumps- may form scabs .
Bartonella Rashes Linear rashes- look like stretch marks but do not follow skin planes Photos taken by Dr. Martin Fried, with thanks to the Lyme Disease Association .
Bartonella Back of legs .
Bartonella Lower back .
Bartonella Under the arm .
Bartonella Mixed rash- Linear and Papular
BARTONELLA-LIKE ORGANISMS TREATMENT- • Fluoroquinolones (for example, Levaquin) are drugs of first choice, and consider adding a proton pump inhibitor • Cell wall drugs ineffective alone, but may synergize with fluoroquinolone • Erythromycins alone totally ineffective, and may inhibit concurrent fluoroquinolone • Rifampin and metronidazole may be alternatives • Response to doxycycline is variable but usually poor • Bactrim may boost effectiveness • Treat for 1 to 3+ months if tolerated .
PIROPLASMS (Babesia species) • Many different species found in ticks (13+). Can test for only B. microti and B. duncani(WA-1) • B. duncani more difficult to treat than B. microti • Diagnostic tests insensitive • Chronic persistent infection documented • Infection is immunosuppressive • Renders Lyme more severe, with more organ damage and more difficult to treat .
BABESIA TESTING • STANDARD SMEARS USEFUL ONLY FOR ACUTE INFECTIONS! • Smears universally negative after two weeks • ENHANCED SMEARS- • Buffy coat • Prolonged scanning, with digital photography • FLUORESCENT IN-SITU HYBRIDIZATION ASSAY • Fluorescent-linked RNA probe • Increases sensitivity 100-fold over conventional Giemsa-stained smears • PCR AND SEROLOGY • ALL METHODS ARE OF LOW YIELD, BUT MAY NOT OVERLAP! .
CLINICAL DIAGNOSIS OF CHRONIC BABESIOSIS • Acute onset of initial illness • Incomplete response to Lyme treatments • Symptoms more severe than expected with Lyme alone • Marked night sweats which may cycle every several days • Air hunger, cough • Severe persistent headaches • Unrelenting fatigue • Off balance- “tippy”, not vertigo • ANY positive test in proper clinical setting .
TREATING BABESIOSIS • Is a parasite, so is not treated with antibiotics • Can be treated while on Lyme medications • Starting points: • Atovaquone (Mepron) 5 cc bid, plus azithromycin 600 mg daily for 4 to 6 months (no doxycycline and no Co-Q 10!) • Malarone (atovaquone + proguanil), 6+ tabs daily • Boosters: • Added sulfur (Bactrim DS), 2 to 4 daily) • Added metronidazole (Flagyl), 750 to 1500 mg/d • Artemesia or artemesenin derivaatives • Alternatives: • Clindamycin + quinine (difficult to tolerate) • Coartem (antimalarial drug new to Babesia treatment) .
EHRLICHIOSIS • Less common than the other tick-borne infections • Acute and chronic forms • Acute- rarely causes a spotted rash • Abrupt onset, high fever, muscle pain, headache, low WBC count, elevated liver enzymes • Chronic- • Headaches and muscle soreness • Persistent leucopenia • Test with serology, PCR or smear • Treat with doxycycline; fluoroquinolones and rifampin are alternatives but may be less effective. • Treat for 2 to 4 weeks .
MYCOPLASMA • “Chronic fatigue” germ • Not clear its origin or source • More often seen in the immunosuppressed • Test with serial PCRs (still insensitive) • Treatment is difficult- antibiotics may not be the only answer. Strengthening the immune system may be the best approach. When antibiotics are used: • Treat with doxycycline and/or a fluoroquinolone, and add hydroxychloroquine (Plaquenil) • Erythromycins & rifampin, with added hydroxychloroquine OK but less effective • Treat for months to years? .
WORMS ! • Dr. Willi Burgdorfer recognized nematodes in ticks decades ago • Dr. Eva Sapi confirmed this last year • Dr. Larry Klapow discovered a new species of nematode in 63-75% of patients from Massachusetts diagnosed with CFIDS • Immunosuppressive so is not picked up with antibody tests and usual markers of parasites (elevated IgE and eosinophilia are absent) • See fatigue as main complaint; also may cause linear or spotted rashes • Transits through the intestinal tract but mainly lives in the lungs • Is treated with a combination of oral and inhaled antiparasite drugs
BIOFILMS • A biofilm is a gel-like substance in which germs can be embedded • Dental plaque is an example of a biofilm • This biofilm gel protects germs from attack by the immune system and by antibiotics • Biofilms in the gut have been implicated in many digestive diseases and possibly food allergies and malabsorption • Metal ions are important components of biofilms (magnesium, iron, others) • Drs. Alan MacDonald and Eva Sapi have shown that Bb forms biofilms, in theory explaining how Bb can persist despite treatment • Dr. Cecile Jadin has found that her patients treated with oral antibiotics do better if they avoid taking oral iron and magnesium supplements until after they are on the antibiotics (OK to give magnesium parenterally)
BIOFILM BUSTERS • In Vitro, the combination of Banderol plus Samento totally dissolved Borrelia biofilms and rendered Bb more susceptible to antibiotic-mediated killing • Marginal further benefit from added enzymes- (Bioluke, nattokinase, etc.) • Chelating out the divalent cations (Mg, Ca, Fe) quite helpful in vitro, but effect not proven in patients
METHYLATION CYCLE • This is a key component of the normal metabolism • Normal operation gives us energy, protects us from free radicals and helps to remove toxins • It has been proven that this cycle can be “blocked” if genetically susceptible people get ill, are overly stressed, or are exposed to excessive levels of toxins • 75% of CFIDS patients who failed to respond to aggressive therapy for CFIDS and Lyme did respond to treatment to remove this methylation cycle block • Treatment consists of a combination of non-prescription supplements given in exceedingly LOW doses and very carefully • Fully 35% had side effects from this treatment, presumably due to sudden release of stored toxins • Also found to be useful in a small study of patients with depression, autism and ADHD
CRAZY, OR IS IT LYME? • When infected, cytokines, the mediators of inflammation, are activated • When this occurs in the CNS, it triggers a diversion of the tryptophan metabolic pathway into kyenurines • The result can be both depression and neurotoxicity • Thus proof that the depression in Lyme can be caused by the infection • In addition, antidepressants are known to decrease levels of the cytokine TNF so at least some of their antidepressant effect may be due to their anti-inflammatory effect.
BORNAVIRUSHanns Ludwig and Liv Bode • Small RNA virus- distant cousin to Rabies and Distemper viruses • Not tick-borne or airborne- only transmitted by close person to person contact, transplacentally or by transfusion • Brain is the site of infection- does not damage nerve cells, but interferes with nerve function • Therefore if can get rid of Bornavirus, there is a full recovery • Bornavirus is present in inactive form in 30% of all individuals tested (Europe) • If chronically ill, severely stressed, or given strong immune suppressing drugs, then virus activates and causes the nerve dysfunction
BORNAVIRUSSymptoms • Adults- initially flu-like symptoms, then fatigue, decreased memory & concentration, and depression • In baby lab animals, also see learning deficiencies • Then develop severe, drug-resistant depression or bipolar disorder • Incidence of active virus is three times higher in moderately or severely depressed patients vs. non-depressed
BORNAVIRUS • TESTING: • Antibody testing and PCR only show exposure, and can be positive in healthy people (latent infection) • If the virus is activated, it enters the blood stream releasing antigen (Ag) and forming circulating immune complexes (CIC) • So, diagnosis of Bornavirus as a cause of illness requires a positive Ag and CIC test • These tests are not available in the USA, but blood samples can be sent to Germany for testing (test has a German patent); in the USA can only get antibody testing- not helpful for diagnosis • TREATMENT: • Antiviral drug AMANTADINE works well- 65% to 70% response rate at 12 weeks (effect begins at 4 weeks) • Dose is 200 to 400 mg daily- check blood level • Treatment can cure infection in those with intact immunity; weakened patients may continue taking amantadine chronically
XMRV • Xenotropic murine leukemia-virus related virus (XMRV) is a gammaretrovirus that was first isolated from prostate cancer patients in 2006 • In 2009 Judy Mikovits found XMRV in CFIDS patients. Of 101 CFIDS samples analyzed by PCR, 68 (67%) contained XMRV sequences but found it in only in 3.7% of healthy controls. 95% of CFIDS cases from another cohort were antibody positive. • In 2010 Alter and Lo confirmed Mikovits’ findings, with even higher % positive (96% in CFIDS patients) • Mikovits and clinical colleagues also found XMRV in fibromyalgia, atypical MS, ALS, Parkinson’s and autism. • In a cohort of severely ill Lyme patients who did not fully recover despite antibiotics, 100% were XMRV + • XMRV, although a simple retrovirus, is immunosuppressive and is capable of persisting, thus raising the possibility that this virus may play a role in chronic Lyme • What came first? Is the immunosuppression from Lyme allowing XMRV to flourish, or is the immunosuppressive effect of XMRV preventing a full recovery from Lyme? • Is XMRV found in ticks?
TREATING XMRV XMRV ACTIVITY IS INITIATED BY CORTISOL, DIHYDROTESTOSTERONE (DHT), AND INCREASED CYTOKINE ACTIVITY. SO: • Begin with full supportive measures • Be sure there is not excessive cortisol and DHT • Can mitigate excessive cortisol with “Cortitrol” (Pharmanex) • Can decrease DHT with beta sitosterol and with prescription drugs (Propecia, Proscar, Avodart) • Decrease cytokine activity without suppressing the immune system • Circumin, artesunate, alpha lipoic acid, ?stem cells • Consider adding prescription anti-retrovirals • AZT, tenofovir and raltegravir are the only ones that XMRV is sensitive to, but are only weakly effective, and must be used in two or three-drug combinations
NERVE HEALING • IVIG is very useful to clear the residual nerve damage that is caused by Lyme. • It not only helps with remyelination, it also heals the disrupted fine, unmyelinated fibers as documented by serial skin punch biopsies. • These damaged fine fibers are the cause of the intractable and severe neurologic pain, as well as the autonomic neuropathy seen in Lyme. • Can also moderate cytokine storm (anti-inflammatory without being immunosuppressive) • IVIG is probably underutilized
BASIC ADVICE • Never any steroids or other immune suppressives! • No smoking at all • Never any alcohol (send your good wine to me) • Diet • Low carbohydrate, low glycemic index • High quality proteins • Maintain hydration- may need mineral supplements