Download

1 / 22
250 likes | 529 Views
Imaging of Small Renal Masses. Mark E. Lockhart, MD, MPH University of Alabama at Birmingham July 28, 2012. Objectives. Discuss basic imaging findings associated with small renal masses Highlight recent radiology recommendations of incidental renal lesions. Renal “ Masses ”.

E N D
Imaging of Small Renal Masses Mark E. Lockhart, MD, MPH University of Alabama at Birmingham July 28, 2012
Objectives • Discuss basic imaging findings associated with small renal masses • Highlight recent radiology recommendations of incidental renal lesions
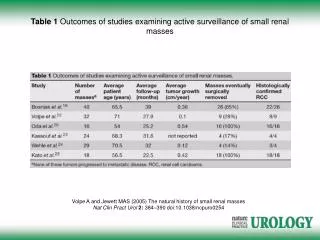
Renal “Masses” • Most are now incidental on US, CT and MRI • Most are simple cysts and require no action • Incidental RCC have lower stage of malignancy (82% stage 1) than symptomatic (37%) Konnak JW, J of Uro 1985; Ozen H, Br J Uro 1993
Column of Bertin • Actually a septum rather than a column • Junction of interpolar region and pole • May be slightly echogenic relative to adjacent cortex
How to evaluate a renal mass • Is it fatty? • Gross fat is less than -20 HU • Consider angiomyolipoma or liposarcoma • Is it cystic? • Is it fluid density (-10 to 20 HU) • Use Bosniak criteria • Does it enhance? • Borderline is 15-20 HU change • Metastases, IVC clot, lymphadenopathy?
Angiomyolipoma • 10% of patients with tuberous sclerosis • 80% of TS have AML • If exophytic then look for wedge of fat in cortex
Bosniak Classification • Bosniak MA.The current radiological approach to renal cysts. Radiology 1986;158:1 -10 • Type 1 – simple cyst • Type 2 – mildly complex; likely benign • Type 3 – complex; worrisome • Type 4 – cystic neoplasm Bosniak MA, Rad 1986 Curry NS, AJR 2000
Bosniak II: Small hyperdense • Cannot show enhancement • Evaluation for de-enhancement can be useful if same scanner on same day
Bosniak IIF • Slightly more complex cysts that cannot be neatly classified as category II or III lesions. • Perceived but nonmeasureable septal enhancement stable on f/u
Bosniak III • Indeterminate cystic masses • Thickened irregular walls or septawith measureable enhancement • 25-59% chance malignancy • Recent work at UAB suggests lower rate • Percutaneous biopsy is controversial Curry NS, AJR 2000; Berland 2012
Bosniak IV • Malignant cystic masses. • 80-100% likelihood of malignancy • Findings similar to Bosniak III but also have enhancing soft-tissue components adjacent to, but independent of, the wall or septum. Bosniak MA, Rad 1986 Curry NS, AJR 2000
Bosniak IV: Thick enhance septa • Multilocular cystic nephroma • Look for extension into collecting system • No venous extension
Renal Cell Carcinoma • Most common renal malignancy • More common in males • Arises in renal cortex – often disrupts renal contour even when small • Bilateral in only 2% • Calcifications in 25-30%
Oncocytoma mimics RCC • Both are solid and disrupt cortical margin • Both can enhance • Both can have central scar
Urothelial Carcinoma • Central renal mass with mild ehancement • Rarely calcified • Extension into collecting system • Nodal metastases
Lipid-Poor AML • Mildly hyperdense on CT • Low T2 signal. Does not drop signal on opposed phase MRI • Enhances similar to RCC
Renal Lymphoma • Focal mass(es) • Infiltrative mass • Renal hilar mass • Perinephric rind • Rarely only site of involvement
Management • ACR white paper on incidental renal masses • Cystic based on Bosniak criteria • Solid based on size • >3cm, surgery • 1-3cm, surgery (may biopsy if hyperdense, homogenously enhancing) • <1cm, observe until 1cm Berland JACR 2010
Management Slight different criteria if high risk patient or limited life expectancy Small mass more likely benign Still rare risk of metastases in small mass Lack of morphologic change over 5 years suggests benign Berland JACR 2010
Management different for VHL Lower malignant potential Resect when largest 3 cm
Acquired Cystic Renal Disease • Much higher risk of RCC development • Consider any solid mass as suspicious
Summary Small renal masses are a common diagnostic challenge A few have characteristic features that can help the diagnosis Know the imaging criteria