Download
1 / 30
340 likes | 578 Views
Depleted Uranium (DU): More than you want to know . . . But what every health physicist ought to know. Ronald L. Kathren, CHP. Ronald L. Kathren, CHP Professor Emeritus Washington State University at Tri-Cities Presented at a breakfast meeting of the Columbia Chapter

E N D
Depleted Uranium (DU):More than you want to know . . . But what every health physicist ought to know Ronald L. Kathren, CHP Ronald L. Kathren, CHP Professor Emeritus Washington State University at Tri-Cities Presented at a breakfast meeting of the Columbia Chapter of the Health Physics Society Richland, WA November 15, 2007 (at the ungodly hour of 7 AM!)
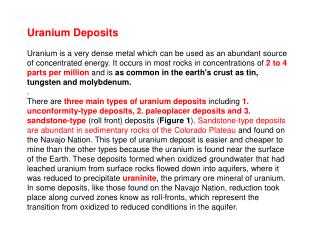
Historical and General Introduction • Human experience with uranium goes back two millennia – the Romans used uranium oxide to impart a yellow color to ceramic glazes • At least as early as the 1400’s, pitchblende, extracted from the Joachimsthal mines, was used to color glass • Uranium was discovered by German chemist Martin Klaproth in 1789; named after planet Uranus
Natural Uranium • A dense (ρ = 18.68 g cm-3), silvery white weakly radioactive and chemically toxic heavy metal • Ubiquitous in the environment (heaviest natural element) • ; NatU contains Three isotopes: U-238 99.27 wt % ~ 50% of activity U-235 0.72 wt % U-234 0.0057 wt % ~ 50% of activity • Several valence states (+4, +5, +6); compounds range fromsoluble(UF6, UCl4) toinsoluble(typically oxides – UO2, UO3, UO4, U3O8 • Pyrophoric – particulates oxidize quickly in air
More History • Uranium metal isolated in 1841 by French chemist Eugene-Melchior Peligot • Radioactivity of uranium was discovered in March 1896 by French physicist Henri Becquerel • Fission of U discovered in 1939 by German chemists Otto Hahn and Fritz Strassmann; process explained by physicists in exile Lise Meitner and Otto Frisch
Toxicological Studies • First toxicological studies by chemist Christian Gmelin (1824); concluded that uranium was “a feeble poison” • Gmelin’s work confirmed by other researchers over the next several decades • Since about 1860 until discovery of insulin in 1920’s used therapeutically to treat diabetes mellitus
Toxicological Studies II • Extensive studies of U toxicity in Manhattan District confirmed low level of toxicity • Low order of toxicity further butressed by studies of accidental exposures and epidemiologic studies of U workers • Use of DU in Gulf Wars and Kosovo generated new interest and intensive study but many questions still remain
Production of Depleted Uranium • A byproduct of the enrichment process • Two basic methods: Gaseous diffusion Gas centrifugation • U-235 content reduced to 0.2 wt % • Specific activity about 60% of NatU • 88.8% of activity from 238U, 9.9% from 234U and only 1.1% from 235U
Uses of Depleted Uranium • Pigments • Industrial catalyst • Counterweight for aircraft control surfaces • Ballast for ships • Radiation shielding • Munitions • Armor
Munitions Usage • High density and self sharpening characteristics provide excellent armor piercing capability • High density and strength also make it excellent for tank armor • DU penetrators produce airborne particulates of typically high fired and hence insoluble DU which fall out close to the point of impact and produce localized ground contamination
Toxicokinetics • Oral absorption poor – few per cent • Percutaneous absorption has not been observed in humans • Absorption following inhalation a function of solubility, particle size; ICRP lung model applies • Approximately 70% of absorbed U is excreted in first 24 hours, largely via urine
Biokinetic Models for Uranium • Several biokinetic models for U have been proposed over last 50 years • ICRP Publication 69 (1995) likely most generally used and accepted model • Other models have been proposed; in general are similar to and basically refinements of ICRP model • Models may not fit well – solubility, route of intake are important factors
Inhaled Uranium • Rely on ICRP lung model • Type F Compounds [UF6, UO2F, UO2(NO3)2] – 100% absorption of fraction not excreted via GI tract with half time of 10 min • Type M Compounds (UO3, UF4, UCl4, U3O8) – 10% absorption of fraction not excreted via GI tract with half time of 10 min; remaining 90% of nonexcreted fraction has half time of 140 days • Type S Compounds (UO2, U3O8) – low and slow absorption – of the fraction not cleared via GI tract, 99.9% absorbed via respiratory tract with half life of 7000 days (~ 19 years) • Note: Some compounds such as U3O8 may behave as Class M or Class S under specific circumstances
Ingested Uranium • Gut absorption poor – f1 = 1-2% for soluble U, order of magnitude less for insoluble forms • ICRP uses 0.02 for soluble forms and 0.002 for highly insoluble forms, the latter specified as UO2 and U3O8. • Gut absorption may be affected by food
Percutaneous Absorption • Not likely – no evidence to support transfer through unbroken human skin • May enter blood through cuts and abrasions • Depositions in wounds may remain for years, slowly releasing U and progeny into systemic circulation; kidney concentration builds up with time
Absorption and Distribution • Once absorbed into systemic circulation, most U is quickly excreted via the kidneys • Small fractions are deposited in skeleton, liver and kidney • Depots may have both long and short term residence compartments
Bioassay for DU • Fecal analysis useful for inhaled material, especially after acute accidental intake • In vivo counting useful; reasonable LLD (few mg) for lung counts • Urinalysis (KPA, ICPMS) most practical and has excellent sensitivity • Hair analysis not established technique and subject to interferences and error • Blood concentration insufficiently sensitive and may not be practical
U is a heavy metal and exhibits heavy metal toxicity Low enrichment U (> ~ 15% U-235) is primarily chemically toxic Toxic effects (including death) have been clearly demonstrated in animals but not in humans – sensitivity variable among species Chemical Toxicity
LD50 • Variable depending on animal species; humans seem to have lower sensitivity to U toxicity than animals • No data for humans, but limited human data and extrapolation from animals suggests that the acute LD50 for ingested or inhaled U is at least several grams
Hard to Believe but True: • There has never been a documented death attributable to U ingestion or inhalation in humans • BUT . . . This does not mean that DU is without toxic effects . . . • More study of DU and its possible effects in man is clearly indicated
Chemotoxic Effects: Kidney • Kidney is the most sensitive organ for chemotoxic effect of DU • Histopathology and apparent mild functional changes may occur days after large acute intakes (tens to hundreds of mg) and manifest as injury to renal tubular epithelial cells • Biomarkers of tubular effects include glucosuria, enzymuria, albuminuria, and elevated blood creatinine or NPN/BUN.
Chemotoxic Effects: Kidney • Threshold for renal effects from acute exposure likely ~ 2 μg U/g kidney but 3μg U/g generally accpted as of now • Effects are typically transient but are more serious and longer lasting with higher exposures • Studies of chronic occupational exposure in workers and Gulf War veterans suggests concentrations > 1μg/g kidney may produce mild tubular dysfunction (Thun et al. 1985; Squibb et al. 2005).
Chemotoxic Effects • Effects on other systems -- CNS, cardiovascular, ocular, liver, immune system -- typically not observed in animal studies or in humans, but any such effects may have been overshadowed and masked by far more severe renal effects • No evidence of reproductive system dysfunction or sperm abnormalities in male Gulf War veterans, nor any evidence of excess fetal abnormalities or mortality. Placental transfer equivocal
Chemical Genotoxicity • Has not been seen (or even looked for) in animal studies • A 10 y followup study of Gulf War veterans classified as ‘high exposure’ based on urine biomarkers was equivocal (McDiarmid et al. 2004) • Recent in vitro studies with Chinese hamster cells suggests chromosome breakage and mutagenicity associated with heavy metals including U (Stearns et al 2005) but such studies have not been confirmed nor are they necessarily applicable to human exposures
Radiation from DU • All three U isotopes in DU are alpha emitters (plus associated photons) • Specific activity of DU = 14.9 kBq g-1 (4.1 x 10-7 Ci g-1 ) • Decay chain products emit betas, photons • Surface dose rate from infinite slab of DU is 2.55 mGy h-1, 90% from beta and 10% from photons
External Exposure Considerations • Potential for significant external exposure is small to zero • Dose rate 10 cm from an infinite slab of DU is only ~ 0.1 mGy h-1 • Unless DU is in contact with the skin (or very nearly so) it is virtually impossible to get a dose sufficient to produce any deterministic effect
Internal Exposure Considerations • Risk of deterministic effects from radiation virtually zero as chemotoxicity effects would be overwhelming and possibly fatal irrespective of route of entry • Ditto for carcinogenic risks from ingestion of soluble DU; ingestion of 1 g of soluble DU produces a total stochastic risk of 3.3 x 10-5 including both carcinogenesis and genetic effects.
Risk from Inhaled DU • Inhalation of soluble DU compounds dose not pose significant stochastic or deterministic risk from radiation: the chemical effects are overwhelming • Inhalation ofinsoluble aerosols may pose significant stochastic risk – e.g. inhalation of 1 mg of a 1 μm AMAD Class S aerosol produces a lifetime stochastic risk of 5.6 x 10-6 primarily from lung cancer • Lung cancer risk may be potentiated or increased by other insults such as smoking
Epidemiology • Numerous radioepidemiologic studies have been done over the past three decades of uranium miners, millers, and workers and of populations exposed to high background levels of U • DU studies are under way in military and civilian populations in areas where DU munitions were used
EpidemiologicFindings • Results are at most equivocal and certainly comforting – no study has shown a statistically significant excess for total cancer (so if there are in fact effects they will be minimal) • No study has shown long term kidney or other somatic effects associated with acute or chronic exposure to uranium