Ritalin ® & AD/HD just calming the troublemaker ???
Ritalin ® & AD/HD just calming the troublemaker ???. Dr.med.Sven Schellberg Global Communications & Brand Manager Psychiatry NOVARTIS Pharma AG, Basel, Switzerland. Don‘t worry, potentially a new Ritalin ® customer. What do these gentlemen have in common ?. ICD-10 versus DSM IV.


Ritalin ® & AD/HD just calming the troublemaker ???
E N D
Presentation Transcript
Ritalin® & AD/HD just calming the troublemaker ??? Dr.med.Sven Schellberg Global Communications & Brand Manager Psychiatry NOVARTIS Pharma AG, Basel, Switzerland
ICD-10 versus DSM IV inattentive Type 314.00 Inattentiveness Impulsivity Disturbed activity (Hyperactivity) hyperkinetic Syndrome F90 combined Type 314.01 hyperactive impulsive Type 314.01
School Delinquency ADHD Occupational status Social/financial status Drug abuse Peer relationships Traffic accidents Marital status
Statistics • 2 - 6 % of pupils (age 6 – 16) show symptoms of AD/HD • Hyperactivity is more common in boys • in 70 % of the patients, symtomatology calms in adolescence • 30 % keep symptoms which need therapy in adulthood
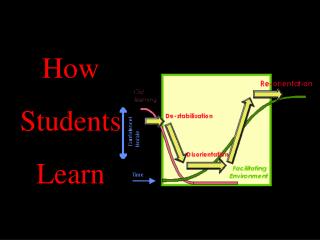
AD/HD Etiology
Etiology • Attention, evaluation of situations, learning and activity are functions which are located in dopaminergic areas of the brain • In animal experiments a depression of dopaminergic function leds to hyperactivity, aggression and worsening of learning procedures
Etiology Krause et al.
Etiology Bush et al.
Etiology Family and Interactions Education Environmental Effects Food
Stroop blackredgreenyellowblueredblackgreenyellow blackredgreenyellowblueredblackgreenyellow blackredgreenyellowblueredblackgreenyellow
AD/HD Diagnosis
Diagnosis • History and anamnesis including interviews with patient, parents, teachers • Symptomatology (differing criterias between DSM IV (AAP) and ICD-10) • Rating Scales (CRS, CBCL etc.) • Exclusion of other medical disorders (e.g. epilepsy, brain damage, schizophrenia, hyperthyreosis) • physical examination including EEG, lab, intelligence testing
AD/HD Treatment
Treatment of AD/HD always has to combine educational, psychotherapeutical and psychopharmacological methods
Stimulants • The use of stimulants started in the 1930‘s when their stimulative effects on the dopamingergic system and their psychotropic effects were discovered • First Amphetamine and Metamphetamine were used • First descriptions of an use of Methylphenidate in „MCD“ in the 1960‘s • Detailed descriptions in the 1980‘s by Wender et al.
Methylphenidate (Ritalin®) Dr.Leando Panizzon & Marguerite („Rita“) Panizzon
Stimulants - Chemistry Amphetamine Mescaline Methylphenidate Dopamine MDMA „Extasy“
Mode of action Krause et al.
AD/HD Because of time one example of efficacy only
Substance Abuse relative risk
Ritalin® LA Product backgrounder and competitors
Facts and Problems • Onset of action after 20 – 40 minutes • Duration of action 2-4 hours • Repeated dosing – often over school-time - mandatory • Acute tolerance requires peaked doses with raising plasma levels over the day and drug free interval at night • Stable plasma levels show poor clinical efficacy, sharp increase in plasma levels in the morning required
Ritalin® LA - Objectives • Fast onset of action in the morning, with a high morning dose • Double peak pharmacokinetic with raising plasma levels over the day • Duration of action about 8 – 10 h to cover schoolday, but not to interfer with sleep at night • Easy to swallow, no food interaction • Easy switch from standard medication • Individualized dosing
Ritalin® LA Ritalin® LA 20 mg (n=19) Markowitz J, et al. Clin Pharmacokinet. In press.
Concerta® - OROS™ Concerta® is a trademark of Janssen Cilag, / J&J
Ritalin® LA vs. Concerta® Concerta® 18 mg (n=19) MPH concentration (ng/mL) Time (h) Ritalin® LA 20 mg (n=19) Markowitz J, et al. Clin Pharmacokinet (2003) 42(4) 1-9
Concerta® Dose strenghts 18, (27), 36, (54) mg Initial dose 22 % Sustained dose 78 % Duration of action up to 12 h Capsule must not be opened Ritalin® LA Dose strenghts 20, 30, 40 mg Initial dose 50 % Sustained dose 50 % Duration of action up to 8 h Capsule may be opened and sprinkled on soft food Important differences Concerta® is a trademark of Janssen Cilag, / J&J
How to switch ? • Switching can be done from day to day • Switching sometimes needs new dose adjustment • Always remind initial 50 % of dose (10 mg, 15 mg, 20 mg) • Starting with too high doses may lead to initial side effects and bad compliance !
Pharmacodynamics Or what does this mean in daily practice ?
School Day Efficacy of Ritalin® LA vs. Concerta® • Randomized, rater blind, placebo controlled clinical trial • 36 children, 6-12 years, 29 boys, 7 girls • All stabilized on 20 mg MPH/die ahead of trial • 4 way crossover design • Study medication on days 7, 14, 21, 28, standard medication in-between • Swanson, Kotkin, Alger M-Flynn, Pelham (SKAMP) Attention/Deportment Scale • Age/intelligence-appropriate, 400-question, 10-minute written math test
Worsening Improvement Ritalin® LA vs. Concerta®SKAMP Attention over first 4 hours Change from Baseline (Predose) 0-4 Hours N=36 Ritalin® LA 20 mg -2.481 *† Concerta®18 mg -1.362 Concerta®36 mg -1.55 1.24 Placebo ‡ *P=0.015 for Ritalin® LA 20 mg vs Concerta® 18 mg. †P=0.043 for Ritalin® LA 20 mg vs Concerta® 36 mg. ‡P<0.001 vs all active treatment groups.
Ritalin® LA vs. Concerta®SKAMP Attention over schoolday Worsening Improvement Change from Baseline (Predose) 0-8 HoursN=36 Ritalin® LA 20 mg -4.481 *† Concerta®18 mg -2.719 Concerta®36 mg -3.244 3.786 Placebo ‡ *P=0.074 for Ritalin® LA 20 mg vs Concerta® 18 mg. †P=0.208 for Ritalin® LA 20 mg vs Concerta® 36 mg. ‡P<0.001 vs all active treatment groups.
Placebo Ritalin® LA 20 mg Ritalin® LA vs. Concerta®SKAMP Combined Concerta® 36 mg N=36 Concerta® 18 mg *† *† *† * Mean change from predose in SKAMP-combined 0.5 1.0 2.0 3.0 4.0 6.0 8.0 0 Time (h) *P<0.05 for Ritalin® LA 20 mg vs Concerta® 36 mg. †P<0.05 for Ritalin® LA 20 mg vs Concerta® 18 mg.
Strattera® (Atomoxetine, Eli Lilly) • Atomoxetine is a norepinephrine-reuptake inhibitor, orginally developed as antidepressant (Pharmacia) • Atomoxetine has no dopaminergic activity • Atomoxetine is the first non-stimulant approved for treatment of AD/HD • Atomoxetine is the first pharmacologic treatment, approved for the use of adult AD/HD • Onset of action as with other antidepressants is delayed (4 – 6 weeks at minimum)
Strattera® (Atomoxetine, Eli Lilly) • Efficacy of Atomoxetine seems to be lower than that of stimulants • Common side effects are nervousness, sleeplesness, loss of appetite, decreased body weight, sexual dysfunction, especially in boys • In US Atomoxetine gained 15 % market share in AD/HD market within 6 months after launch • Approval and launch in EU has been delayed several times – expected currently for H2/2004
What about the critics ? Scientology™