Download
1 / 13
130 likes | 317 Views
SNOMED and Veterinary Clinical Systems. “Do we have to eat the whole elephant?”. Dr. Jeff Wilcke, June 2008. Veterinary medicine without standards. We like things as they are. We only need our own information.

E N D
SNOMED and Veterinary Clinical Systems “Do we have to eat the whole elephant?” Dr. Jeff Wilcke, June 2008
Veterinary medicine without standards We like things as they are. We only need our own information.
Missed Opportunities: Veterinary medicine without (information) standards (assumes organizations wish to share information). • We cannot reliably aggregate, collate and analyze data. • We cannot transmit information reliably. • We throw away information that might lead to better patient care, increased profitability, improved biosecurity, etc… • We cannot integrate external sources of information into patient care (e.g. Structured Product Label) • We cannot reliably contribute to pools of biomedical data (i.e., Adverse reaction reporting; clinical trials; evidence-based medicine).
Are standardized nomenclatures needed? • I must declare a conflict of interest • It is not possible to answer this question without evaluating the precise nature of the activity. • It is likely that different activities will require different capabilities of the nomenclature(s).
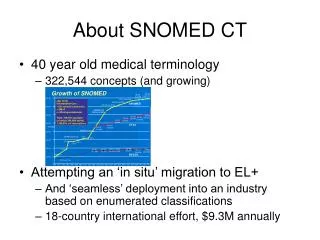
Why big and complicated? • Medicine is big and complicated. • Even simple lists of the logical concepts required to describe narrow fields can be tens of thousands of concepts. • Rule #1 for terminology: Content, content, content • To leverage the information from the data, analysis must be directed by logic. • Logic embedded in SNOMED relationships drives queries. • Stakeholder satisfaction with data analysis includes management of synonomy. • Rarely a feature of simple appealing terminologies.
Why does veterinary medicine need a terminology as big and complicated as SNOMED? • Because nobody is paying us to participate in more than one, and SNOMED is the only general terminology that has significant general veterinary content (especially as concern breadth of species coverage). • Various specializations of Veterinary medicine have both overlapping and independent terminology needs. • Solving problems that create initial resistance to standardized terminology require sophisticated solutions (e.g. synonomy)
Implementation strategies (Philosophy) • Solve small tractable problems with robust technologies. • Robust so you can grow the solution to solve additional and larger problems. • Why? • Because NOBODY has successfully implemented SNOMED as an “interface” terminology in an entire medical record. • Build political momentum and confidence in the project with small inexpensive “wins” (Walk before you attempt to run)
We don’t really want big and complicated so how can SNOMED be implemented in a veterinary medical information system? • Subsets (using SNOMED for data entry) • Use no more of SNOMED than you need. • Portions of SNOMED are going to be irrelevant to any particular purpose. • Entire hierarchies may be isolated (you may not want your system to display substances when abstracting a diagnosis of poisoning). • Subsets need to be small • Even whole hierarchies are completely overwhelming from a data-entry point of view. • (e.g. all possible veterinary findings)
Implementation strategies • Subsets • Build SNOMED subsets as interface • Use medical records staff to “capture” interface subsets. • Existing Interface terminology likely already in rough (at least) concept subsets. • Map existing interface to SNOMED for communications and analysis.
Pitfalls in implementation • Faulty assumptions about what the problem (with terminology) IS… • Believing that the hardest problem is technological. • Believing that the meaning of the concepts your medical must communicate is unimportant to success.
Pitfalls in implementation • Believing that any list of concepts (words and phrases) is ever long enough • Believing that the big terminology hurdle is about importing the right technology. • Failing to recognize that a nomenclature does not require ongoing maintenance. • Believing that simple lists can reliably convey medical knowledge.
How does SNOMED affect the everyday user of computer software • Done correctly, the everyday user should be completely oblivious to the existence of SNOMED.
SNOMED vs a proprietary nomenclature Do you intend to communicate with the government (FDA, USDA) electronically? Do you intend to integrate electronic drug labels in your systems? Planning for e-radiology and/or PACS? Is it important that your information “plays well with others” ?