Download
1 / 24
300 likes | 380 Views
Pituitary apoplexy is a sudden-onset condition often due to pituitary tumor hemorrhage or infarction. Learn about its pathophysiology, clinical features, predisposing factors, and imaging studies. Sheehan syndrome is a specific form postpartum.

E N D
Pituitary apoplexy Int 李明吉
Introduction • The word "apoplexy" comes from the Greek "apoplexia" meaning a seizure, in the sense of being struck down. In Greek "plexe" is "a stroke." The ancients believed that someone suffering a stroke had been struck down by the gods • apoplexy :a sudden neurologic impairment, usually due to a vascular process
Introduction • Pituitary apoplexy : --sudden onset of headache --visual symptoms (VF&VC:optic nerve or chiasm Ocular motility:cranial nerves in cavernus sinus ) --altered mental status --hormonal dysfunction • There is usually an existing pituitary adenoma present.
Pathophysiology -- stems from an acute expansion of a pituitary adenoma or, less commonly, in a nonadenomatous gland, from infarction or hemorrhage. -- Some postulate : gradual enlarging pituitary tumor compressing and distorting the hypophyseal stalk and its vascular supply causing ischemia and subsequent necrosis -- Another theory :rapid expansion of the tumor outstrips its vascular supply resulting in ischemia and necrosis (doubtful? tumors that undergo apoplexy are slow growing)
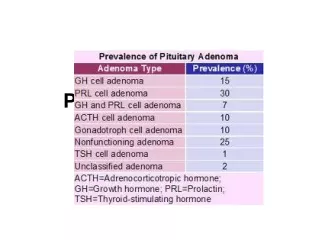
Frequency: This condition results in an estimated 1.5-27.7% of cases of pituitary adenoma • Sex: Male-to-female predominance is 2:1. • Age: The age range is 37-57 years.
Clinical manifestations • headache in 95% of cases. • The headache is sudden .Frequently, it is retro-orbital in location and may be unilateral at onset, then becomes generalized. • Vomiting occurs in 69% of patients and often accompanies the headache.
Clinical manifestations • The classic visual field defect is a bitemporal superior quadrantic defect. • Ocular paresis (78%) results from compression of the cavernous sinus, which make cranial nerves III, IV, VI vulnerable to compression. • diplopia may be present. • Of the cranial nerves, the oculomotor nerve is involved most commonlyunilateral dilated pupil, ptosis, • Less commonly, cranial nerve IV is involved
Clinical manifestations • Horner syndrome may develop from damage to the sympathetic fibers. • Involvement of the hypothalamus may alter thermal regulation. • Destruction of adenohypophyseal tissue may lead to endocrinologic deficiencies.
Predisposing factors • Predisposing factors :endocrine stimulation tests, bromocriptine treatment, head trauma, pregnancy, and pituitary irradiation. • Some believe :more prevalent in patients who produce excess pituitary hormones (eg, acromegaly, Cushing syndrome) because the tumor is fueled by the hormones. Others :most pituitary tumors that undergo apoplexy are endocrinologically silent.
Sheehan syndrome • Sheehan syndrome refers to pituitary apoplexy of a nontumorous gland, presumably due to postpartum arterial spasm of arterioles supplying the anterior pituitary and its stalk. • In 1937, Sheehan reported 11 cases of women who died in the puerperium -- 11/11 necrosis of the anterior pituitary gland -- 9/11severe hemorrhage at delivery. -- 2/11 no hemorrhage but were gravely ill prior to delivery. • The pituitary gland hypertrophies in pregnancy. This hypertrophy combined with locally released factors mediate vascular spasm more susceptible to infarction from compromised blood flow.
Sheehan syndrome • inability to lactate (prolactin deficiency ) amenorrhea (gonadotrophin deficiency), skin depigmentation. • hypothyroidism hypoadrenalism diabetes insipidus(posterior pituitary involvement)
Imaging Studies • CT scan and MRI. • MRI is the most sensitive imaging study for evaluating the pituitary gland, possibly visualizing hemorrhage not seen on CT scan. • In the first 3-5 days, hemorrhage within the sella is isointense or hypointense on T1-weighted images. On T2-weighted sequences, the blood appears hypointense.
Imaging findings • CT: CT(-): -acute: sellar/suprasellar mass with patchy or confluent hyperdensity,may assocciated with SAH -chronic:’’empty sella’’(filled with CSF) CT(+):minimal or no enhancement (rim-pattern suggestive of PA)
Imaging findings • MR: T1:early acute, enlarged gland, iso/hypointense with brain late acute/subacute:hyperintense chronic:hypointense T2:acute: enlarged, hypointense (hemorrhagic) or hyperintense (nonhemorrhagic) pituitary subacute:hyperintense Chronic:hyperintense T1+:rim enhancement
case • 69 y/o male • Headache, vomitting • L’t ptosis, L’t EOM limitation(medial) • Feverantibiotics , subsided after steroid usage • Ptosis persistenttransfer to NS for operation • Pathology report:pituitary adenoma
case • CT(-):a sellar lesion with slight high density • CT(+):without obvious intra-lesion enhancement.
case T2 T1 T1 GD+ • mixed signal intensity on T1W, T2W images. Hematoma content is suspected. Mild contrast enhancement.
46-year-old man , - sudden onset of severe headache - nonprojectile vomiting, - followed by high fever and cranial nerve palsies • a large heterogeneous mass, highly consistent with a hemorrhagic macroadenoma Infect Med 17(12):806,810,811, 2000 Pituitary Apoplexy: An Overlooked Cause of Fever and CNS Abnormalities
T2 and FLAIR :heterogeneity of signal, consistent with hemorrhage and or proteinaceous debris.
Post contrast T1: no detectable enhancement. • The normal calibler left cavernous carotid (first image) • narrowed right cavernous carotid (following 3 images w/arrows).
Treatment • Administer high-dose corticosteroids (most patients have hypopituitarism). Hydorcortisone100 mg IV initially, then q6-8h until surgery • evaluate electrolytes, glucose, and pituitary hormones • Administer appropriate endocrinologic replacement therapy alone or combined with transsphenoidal surgical decompression of the tumor
參考資料 • Emedicine-pituitary apoplexy,January 27, 2005 • Diagnostic imaging-Brain • Wake Radiology website • Infect Med 17 Pituitary Apoplexy: An Overlooked Cause of Fever and CNS Abnormalities