Download
1 / 47
490 likes | 741 Views
The ABCs of Chest X-Rays in Trauma. Joe Lex, MD, FACEP, MAAEM Temple University School of Medicine Philadelphia, PA USA. How Accurate Is Chest X-Ray?. Portable erect AP for detecting serious injuries: 78.7% sensitive Portable supine: 58.3% sensitive Missed (n=100) Bony injuries: 5

E N D
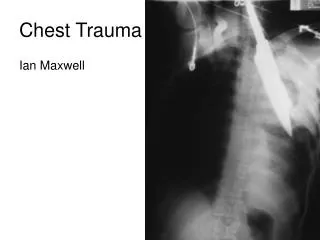
The ABCs of Chest X-Rays in Trauma Joe Lex, MD, FACEP, MAAEM Temple University School of Medicine Philadelphia, PA USA
How Accurate Is Chest X-Ray? Portable erect AP for detecting serious injuries: 78.7% sensitive Portable supine: 58.3% sensitive Missed (n=100) Bony injuries: 5 Pneumothorax: 1 Hemothorax: 7 ABC • Pulmonary contusion: 1 • Diaphragm rupture: 1 Hehir MD. Aust N Z J Surg 60(7):529, July 1990
Additional Value of CT Pulmonary contusion: 15% Pneumothorax: 12% Hemothorax: 8% Rib fracture: 8% Aortic abnormalities: 4% Mediastinal hematoma: 3% Spine fracture: 3% ABC Omert L, et al. Am Surg 7:660, July 2001
Traumatic Aortic Rupture 90% of ruptures at aortic isthmus 4% at branch vessels Chest x-ray 10% PPV 98% NPV ABC
Traumatic Aortic Rupture Nasogastric tube deviated to right Left main stem bronchus depressed Mediastinum wide Aortic arch obscured or irregular Left apical cap Aorto-pulmonic window opacified Trachea deviated to right 1st or 2nd ribs fractured ABC
Traumatic Aortic Rupture Direct radiographic signs Aorta caliber change Intraluminal irregularity Abnormal contour: perivascular hematoma ABC
Traumatic Aortic Rupture Rapid increase in size of the aorta on serial chest films Double shadow of aortic arch Intimal calcifications displaced by more than 6 mm (“calcium sign”) Tracheal deviation Left pleural effusion ABC
Traumatic Aortic Rupture 86 patients; rupture in 15% Only signs associated with TAR: NG tube deviation and left mainstem bronchus depression Useful combination: NG tube / tracheal deviation, loss of aortic contour, loss of aortic knob ABC Marnocha HE. Am J Roent 144(1):19, 1985
Traumatic Aortic Rupture No NG / tracheal deviation, loss of aortic contour, loss of aortic knob: 0% prevalence All but one with TAR had at least three signs Three of four signs also present in four patients without TAR ABC Marnocha HE. Am J Roent 144(1):19, 1985
Traumatic Aortic Rupture ABC Apical cap
Traumatic Aortic Rupture? Mediastinal hematoma without aortic rupture ABC
How Wide Is Wide? 8.0 to 8.8 cm upper limit: x-ray techniques employed in 1970s Mean mediastinal width: 6.31 cm Average depth of board: 4.5 cm Distance between board and x-ray cassette beneath 6 different types of gurneys: 7.1 cm – 12.9 cm ABC Gleeson CE, et al. Emerg Med J 18:183, 2001
How Wide Is Wide? Varies: Focus-to-Film Distance (FFD), cassette placement FFD 100 cm with cassette directly under patient (1970s): mean mediastinal width 7.5cm FFD 140 cm with cassette under spinal board: upper limit 9.68 cm. ABC Gleeson CE, et al. Emerg Med J 18:183, 2001
Traumatic Aortic Rupture High-speed deceleration injury or side impact Multiple rib fractures or flail chest Pulse deficits Hypertension Systolic murmur over back Hoarseness without laryngeal injury Superior vena caval syndrome ABC
Seat Belt Marks ABC
Seat Belt Marks ABC
Seat Belt Marks ABC
How Wide Is Wide? Subjective interpretation of mediastinal widening more reliable than direct measurement ABC Lee FT Jr, et al. J Emerg Med 11:289, 1993.
What Sign Is Best? Most sensitive Wide mediastinum Obscured aortic knob ABC Gleeson CE, et al. Emerg Med J 18:183, 2001
What Sign Is Best? Most specific Opacified clear space between aorta and pulmonary artery Displaced NG tube Widened paratracheal stripe Widened right paraspinal interface ABC Gleeson CE, et al. Emerg Med J 18:183, 2001
Bronchial Fracture In 1.5% major chest trauma 30% missed 80% within 2.5 cm of carina ABC Ramzy AI, et al. J Trauma. 1988 Sep;28(9):1353-7.
Bronchial Fracture 4 P’s: Persistent or Progressive Pneumothorax or Pneumomediastinum ABC
Bronchial Fracture ABC One tube…
Bronchial Fracture ABC Two tubes…
Bronchial Fracture Lung collapses toward bottom of chest cavity (“fallen lung”) ABC Wintermark M, et al. Eur Radiol. 2001;11(3):409-11.
Bronchial Fracture ABC Bronchial stenosis after undetected tear
Bronchial Fracture Diagnosis: bronchoscopy ABC
Cord Injury ABC
Cord Injury ABC
Cord Injury Occurs in 3% major BCT 12% neurologically intact Thoracic facets face inward Lumbar facets face outward Critical location for fracture / dislocation / subluxation: T9 – T10 – T11 ABC van Beek EJ, et al. Injury. 2000 May;31(4):219-23.
Cord Injury Rule of 2’s Maximum 2 mm difference for… …interspinous space …interpedicular distance …intrapedicular distance ABC
Cord Injury Rule of 2’s Maximum 2 mm … …interspinous space …interpedicular distance …intrapedicular distance ABC
Rule of 2’s: Maximum 2 mm difference in interpedicular distance on Antero-Posterior film Cord Injury ABC
Cord Injury / Thoracic Spine Thoracic spine fractures emulate aortic rupture Mediastinal widening Left apical cap Deviated NG ABC Bolesta MJ, et al. J Bone Joint Surg Am. 1991 Mar;73(3):447-50.
Pneumothorax PTX
Pneumothorax Subtle signs on supine x-ray Deep sulcus Sharp cardiac borders Basilar hyperlucency Visualized pericardial fat tags PTX
Pneumothorax Do we need both Inspiratory and Expiratory films? 233 patients with suspected pneumothorax Initially diagnosed in 54 Paired inspiratory and expiratory films increased accuracy by 8% PTX Aitchison F. Arch Emerg Med 10(4):343, 1993
Pneumothorax Chest x-ray after tube placement PTX
Pneumothorax Chest CT after tube placement PTX
Pneumothorax 2.5-cm margin of gas peripheral to the collapsing lung corresponds to a pneumothorax of about 30% 400ml of blood may obliterate only the costophrenic angle PTX