Download
1 / 96
960 likes | 1k Views
Understand the incidence, characteristics, classification, and histologic features of CNS tumors. Learn about the major classes of brain tumors and their clinical implications.

E N D
Central Nervous System Tumors Doç. Dr. A. Işın DOĞAN-EKİCİ Department of Pathology
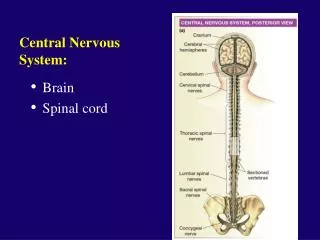
The annual incidence of tumors of the CNS 10 to 17 per 100,000 persons for intracranial tumors 1 to 2 per 100,000 persons for intraspinal tumors; half to three-quarters are primary tumors, the rest are metastatic. Tumors of the CNS account for 20% of all cancers of childhood. Seventy per cent of childhood CNS tumors arise in the posterior fossa; a comparable number of tumors in adults arise within the cerebral hemispheres above the tentorium Incidence of CNS Tumors
Tumors of the nervous system have several unique characteristics that set them apart from neoplastic processes elsewhere in the body. 1- The distinction between benign and malignant lesions is less evident in the CNS than in other organs. Some glial tumors with histologic features of a benign neoplasm, including low mitotic rate, cellular uniformity, and slow growth, may infiltrate large regions of the brain, thereby leading to serious clinical deficits and poor prognosis. 2-The ability to surgically resect infiltrating glial neoplasms without compromising neurologic function is limited.
3-The anatomic site of the neoplasm can have lethal consequences irrespective of histologic classification; for example, a benign meningioma, by compressing the medulla, can cause cardiorespiratory arrest. 4-The pattern of spread of primary CNS neoplasms differs from that of other tumors: Even the most highly malignant gliomas rarely metastasize outside the CNS. The subarachnoid space provides a pathway for spread, so seeding along the brain and spinal cord can occur in highly anaplastic as well as in well-differentiated neoplasms that extend into the CSF pathways.
The four major classes of brain tumors are: • Gliomas • Neuronal tumors • Poorly differentiated neoplasms • Meningiomas
Gliomas, derived from glial cells, include: • astrocytomas, • oligodendrogliomas, • ependymomas.
Astrocytomas Several different categories of tumors derived from astrocytes are recognized, including: • fibrillary astrocytoma, • glioblastoma, • pilocytic astrocytoma, and • pleomorphic xanthoastrocytoma • other rarer types. These have characteristic histologic features, distribution within the brain, age groups typically affected, and clinical course.
Fibrillary (Diffuse) Astrocytomas and Glioblastoma • Incidence: 80% of adult primary brain tumors. • found in the cerebral hemispheres (also occur in the cerebellum, brainstem, or spinal cord) • Age: 40-60 y • Most common presenting signs and symptoms: seizures, headaches, and focal neurologic deficits • Fibrillary astrocytomas show a spectrum of histologic differentiation that correlates well with clinical course and outcome.
Diffuse fibrillary astrocytomas can be well differentiated (astrocytoma) or less differentiated (higher-grade), ranging from anaplastic astrocytoma to glioblastoma. • macroscopic appearance: • poorly defined, • gray, • infiltrative tumor • expands and distorts the invaded brain
These tumors range in size from a few centimeters to enormous lesions that replace an entire hemisphere. • The cut surface: either firm or soft and gelatinous; cystic degeneration may be seen. • In glioblastoma, variation in the gross appearance of the tumor from region to region is characteristic: Some areas are firm and white, others are soft and yellow (the result of tissue necrosis), and yet others show regions of cystic degeneration and hemorrhage
microscopic examination: • well-differentiated fibrillary astrocytomas are characterized by: • a mild to moderate increase in the number of glial cell nuclei, • variable nuclear pleomorphism, • intervening feltwork of fine, GFAP-positive astrocytic cell processes that give the background a fibrillary appearance. • Anaplastic astrocytomas show regions that are more densely cellular and have greater nuclear pleomorphism from well-differentiated fibrillary astrocytoma; mitotically active cells are often observed.
Gemistocytic astrocytoma • tumors in which the predominant neoplastic astrocyte shows a brightly eosinophilic cell body from which emanate abundant, stout processes.
Glioblastoma • Glioblastoma (previously called glioblastoma multiforme) has a histologic appearance similar to anaplastic astrocytoma + additional features of necrosis and vascular or endothelial cellproliferation, each of which often has a stereotypic appearance. • Necrosis in glioblastoma, often in a serpentine pattern, occurs in areas of hypercellularity with highly malignant tumor cells crowded along the edges of the necrotic regions, producing a histologic pattern referred to as pseudopalisading
Vascular cell proliferation is characterized by tufts of piled-up vascular cells that bulge into the vascular lumen; the minimal criterion for this feature of glioblastoma is a double layer of endothelial cells. • When vascular cell proliferation is extreme, the tuft forms a ball-like structure, the glomeruloid body. • Vascular endothelial cell growth factor (VEGF), produced by malignant astrocytes, perhaps in response to hypoxia, contributes to this distinctive form of vascular change. • gliomatosis cerebri: multiple regions of the brain, in some cases the entire brain, are infiltrated by neoplastic astrocytes
Grading Scheme of CNS neoplasms: • World Health Organization (WHO) grading scheme based on their biologic behavior, ranging from grade I to grade IV. • tumor grade is expressed in the format "x/IV." • For diffuse fibrillary astrocytomas, the most recent WHO scheme separates these tumors into well-differentiated astrocytoma (grade II/IV), anaplastic astrocytoma (III/IV), and glioblastoma (IV/IV).
Molecular Genetics • Among the alterations that are most commonly found in the low-grade astrocytomas are inactivation of p53 and overexpression of PDGF-A and its receptor. • The transition to higher-grade astrocytoma is associated with additional disruption of tumor-suppressor genes, the RB gene, the p16/CDKNZA gene, and a putative tumor suppressor on chromosome 19q.
Clinical Features. • The presenting symptoms of astrocytomas depend, in part, on the location of the tumor and its rate of growth. • Astrocytomas have a tendency to become more anaplastic with time. • With well-differentiated astrocytomas, the symptoms may remain static or progress only slowly over a number of years, with a mean survival of more than 5 years. • Patients usually have more rapid clinical deterioration that is generally correlated with the appearance of anaplastic features and more rapid growth of the tumor. • The prognosis for patients with glioblastoma is very poor. • only 8 to 10 months; fewer than 10% of patients are alive after 2 years.
Pilocytic Astrocytoma • Pilocytic astrocytomas are distinguished from the other types by their pathologic appearance and relatively benign behavior. • typically occur in children and young adults • usually located in the cerebellum but may also appear in the floor and walls of the third ventricle, the optic nerves, and occasionally the cerebral hemispheres.
PILOCYTIC ASTROCYTOMA(GRADE I) WELL-DEFINED, HOMOGENEOUSLY ENHANCING MASS
macroscopic examination: • a pilocytic astrocytoma is often cystic, with a mural nodule in the wall of the cyst. • If solid, it may be well circumscribed or, less frequently, infiltrative. • microscopic examination: • the tumor is composed of bipolar cells with long, thin "hairlike" processes that are GFAP-positive; • Rosenthal fibers, • eosinophilic granular bodies, • microcysts are often present. • increase in the number of blood vessels, often with thickened walls or vascular cell proliferation, • necrosis and mitoses are uncommon. • Unlike diffuse fibrillary astrocytomas of any grade, pilocytic astrocytomas have a narrow infiltrative border with the surrounding brain.
These tumors grow very slowly, are considered as WHO grade I/IV, • in the cerebellum particularly, may be treated by resection. • Symptomatic recurrence from incompletely resected lesions is often associated with cyst enlargement rather than growth of the solid component. • Tumors that extend into the hypothalamic region from the optic tract can have a more difficult clinical course because of location. • The histologic separation of these tumors from other astrocytomas is supported by genetic studies; • pylocytic astrocytomas rarely have p53 mutations or other changes found in diffuse fibrillary astrocytomas.
PILOCYTIC ASTROCYTOMA(GRADE I) Reticulin stain demonstrating vascularity of PA
Pleomorphic Xanthoastrocytoma • occurs most often relatively superficially in the temporal lobe of children and young adults, usually with a history of seizures. • survival rate 80% at 5 years. • This is usually a low-grade tumor (WHO grade II/IV) • microscopic examination: • tumor consists of neoplastic, occasionally bizarre, astrocytes, which are sometimes lipidized. • nuclear atypia • abundant reticulin deposits, • relative circumscription • chronic inflammatory cell infiltrates along • absence of necrosis and mitotic activity • Necrosis and mitotic activity are markers of a more anaplastic form, with a correspondingly more aggressive course.
Brainstem Glioma • A clinical subgroup of astrocytomas • occur mostly in the first two decades of life and make up about 20% of primary brain tumors in this age group. • Several distinct anatomic patterns have been defined in the pediatric age group, with differences in clinical course: • intrinsic pontine gliomas (the most common, with an aggressive course and short survival); tumors, often exophytic, arising in the cervicomedullaryjunction region (with a less aggressive course); • tectal gliomas (with an even more benign course and which are rarely biopsied). • Among the rarer brainstem gliomas affecting adults, most are intrinsic pontine gliomas. • These can be separated into low-grade diffuse fibrillary astrocytomas and glioblastoma, with the expected differences in clinical course and survival.
Oligodendroglioma • 5% to 15% of gliomas • most common in the fourth and fifth decades. • Patients may have had several years of neurologic complaints, often including seizures. • The lesions are found mostly in the cerebral hemispheres, with a predilection for white matter. • WHO grade II/IV lesions.
Macroscopy: • oligodendrogliomas are well-circumscribed, • gelatinous, gray masses, • often with cysts, focal hemorrhage, and calcification. • Microscopy: • composed of sheets of regular cells with spherical nuclei containing finely granular chromatin (similar to normal oligodendrocytes) surrounded by a clear halo of cytoplasm. • contains a delicate network of anastomosing capillaries. • Calcification, present in as many as 90% of these tumors, ranges from microscopic foci to massive depositions. • As the tumor cells infiltrate cerebral cortex, there is often formation of secondary structures, particularly with perineuronal satellitosis. • Mitotic activity is usually very difficult to detect, and labeling indices are low.
OLIGODENDROGLIOMA ADULTS (4-5th decades) SLOW GROWING BLEED CALCIFICATION
OLIGODENDROGLIOMA(GRADES II-III) POACHED-EGG CELLS
Anaplastic oligodendrogliomas • (WHO grade III) • characterized by increased cell density, • nuclear anaplasia, • increased mitotic activity, • necrosis. • These changes can often be found in nodules within an otherwise grade II/IV oligodendroglioma. • Also often present in these higher-grade lesions are discrete round cells with cytoplasmic GFAP and nuclei that resemble the other elements of the tumor. • These microgemistocytes differ from gemistocytic astrocytes because they lack abundant processes; the intermediate filaments are restricted to a small lump of cytoplasm.
Molecular Genetics: • The most common genetic alterations in oligodendrogliomas are loss of heterozygosity for chromosomes 1p and 19q. • Additional genetic alterations tend to accumulate with progression to anaplastic oligodendroglioma. The more common of these include loss of 9p, loss of 10q, and mutation in CDKN2A. • Tumors with loss of 1p and 19q but without other alterations have a consistent and long-lasting response to therapy (chemotherapy and radiation). • Those with additional genetic changes have a shorter-lived response, and those without loss of 1p and 19q appear to be refractory to these therapies
Clinical Features • patients with oligodendrogliomas have a better prognosis than do patients with astrocytomas. • Current treatment with surgery, chemotherapy, and radiotherapy has yielded an average survival of 5 to 10 years. • Patients with anaplastic oligodendroglioma have a worse prognosis, although there are subgroups of tumors, as defined by genetic alterations, that respond well to therapy.
The terms oligoastrocytomaand anaplastic oligoastrocytoma have been employed to designate neoplasms consisting of distinct regions of oligodendroglioma and astrocytoma of appropriate grade. • The diagnostic criteria for these entities remain controversial; genetic analysis has not clarified the issue, as tumors with these histologic descriptors can be found that share alterations with either astrocytomas or oligodendrogliomas. • The idea that these tumors are not a true mixture is supported by the observation that the genetic changes are usually of one type or another (1p/19q vs. p53/chr17)
Ependymoma and Related Paraventricular Mass Lesions • Ependymomas most often arise next to the ependyma-lined ventricular system, including the obliterated central canal of the spinal cord. • In the first two decades of life, they typically occur near the fourth ventricle and constitute 5% to 10% of the primary brain tumors in this age group. • In adults, the spinal cord is their most common location; tumors in this site are particularly frequent in the setting of neurofibromatosis type 2
Morphology. • In the fourth ventricle, ependymomas are typically solid or papillary masses extending from the floor of the ventricle • microscopic examination: • composed of cells with regular, round to oval nuclei with abundant granular chromatin. • Between the nuclei, there is a variably dense fibrillary background. • Tumor cells may form gland-like round or elongated structures (rosettes, canals) that resemble the embryologic ependymal canal, with long, delicate processes extending into a lumen more frequently present are perivascular pseudorosettes in which tumor cells are arranged around vessels with an intervening zone consisting of thin ependymal processes directed toward the wall of the vessel. • WHO grade II/IV lesions, • anaplastic ependymomas occur with increased cell density, high mitotic rates, areas of necrosis, and less evident ependymal differentiation. (WHO grade III/IV).
EPENDYMOMA CHILDHOOD/ADOLESCENCE VENTRICLES SPINAL CORD
Myxopapillary ependymomas • distinct but related lesions that occur in the filum terminale of the spinal cord and contain papillary elements in a myxoid background, admixed with ependymoma-like cells. • Cuboidal cells, sometimes with clear cytoplasm, are arranged around papillary cores containing connective tissue and blood vessels. • The myxoid areas contain neutral and acidic mucopolysaccharides. • Prognosis depends on completeness of surgical resection; if the tumor has extended into the subarachnoid space and surrounded the roots of the cauda equina, recurrence is likely
Molecular Genetics • alterations at NF2 gene on chromosome 22 may be involved in the pathogenesis of ependymomas in the spinal cord but not at other sites. • Ependymomas do not appear to share the genetic alterations that are found in other gliomas, such as mutations in p53.
Clinical Features. • Posterior fossa ependymomas often manifest with hydrocephalus secondary to progressive obstruction of the fourth ventricle rather than invasion of the pons or medulla. • Prognosis is poor despite the slow growth of the tumor and the usual lack of histologic evidence of anaplasia. • Because of the relationship of ependymomas to the ventricular system, CSF dissemination is a common occurrence. • An average survival of about 4 years after surgery and radiotherapy has been reported. The clinical outcome for completely resected supratentorial and spinal ependymomas is better