Download
1 / 28
300 likes | 677 Views
Female reproductive system. Female sex hormones. Steroids hormones. Synthesized from cholesterol precursor. Converted from one to the other in the appropriate times which have the required enzymes. Produced in the ovaries mainly but the adrenal cortex produce minimal amounts.

E N D
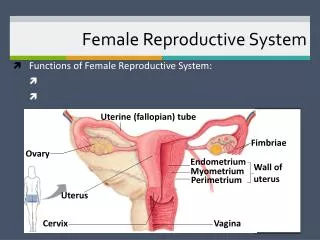
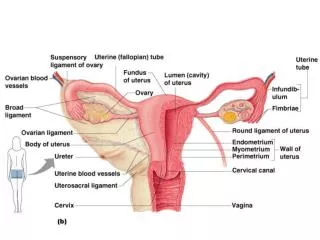
Female sex hormones • Steroids hormones. • Synthesized from cholesterol precursor. • Converted from one to the other in the appropriate times which have the required enzymes. • Produced in the ovaries mainly but the adrenal cortex produce minimal amounts. • In the blood they are transported to target tissues bound to serum protein.
Mechanism of action It bound to carrier protein. Then, it attached to specific receptors on the cell membrane. They enter cell and become bound to a cytoplasm protein receptor and form a steroid protein complex which attached to the nucleus and stimulate the RNA synthesis which stimulate protein synthesis and regulate cell functions.
Oestrogen • Steroid hormone. • Found in the circulation in three forms: 17B oestradiol, oestriol and oestrone. Oestradiol is the most effective (most active compound). • It bound to plasma proteins (albumin and globulin). • Sources from granulosa cells in the ovaries, also from the placenta during pregnancy. • It metabolized in the liver by conjugation with glucoronic acid and excreted in urine.
Actions of oestrogens • Ovarian oestrogen which secreted at puberty responsible for development of secondary sexual characters. • Target tissues include the genitalia, the uterus, the breasts and subcutaneous fats.
Secondary sexual characters • Distribution of fat (body contour) – it causes deposition of subcutaneous fat beneath the breasts, around the hips, thigh and in the gluteal region, which gives the female body the rounded outline. • The breast – it promote the growth of the duct system and slight pigmentation of the areola. • Pubic hair distribution – pubic hair has horizontal top in females (between 12 and 17 years of age). The axillary hair appears at the same time as pubic hair.
Cutaneous gland development – axillary and pubic apocrine glands begin to function at the same time that pubic and axillary hair appear which cause change in body odour. The sebaceous gland secretion becomes thicker which predisposes to blockage or acne, sweat glands of the body become more active. • General growth is promoted by its anabolic action which causes closure of the epiphysis and limit skeletal growth. • During the menstrual cycle, oestrogen responsible for proliferation of the endometrium, it induces the growth of uterine muscle and increase the blood flow in the uterus.
Cyclic oestrogen secretion results in regulation of gonadotrophic hormone where: • GnH (FSH and LH) are secreted in a cyclic pattern during the female reproductive life (they regulate the menstrual cycle). • FSH and LH feedback on the anterior pituitary. • High level of oestrogen has negative feedback on the hypothalamic pituitary axis by inhibiting FSH, but has little effect on LH.
In mid-cycle, high level of oestrogen induces LH surge (positive feedback) also progesterone feedback at the mid-cycle to enhance LH surge. • In the luteal phase, high level of progesterone acts with oestrogen to inhibit gonadotrophin secretion (negative feedback). • The use of oestrogen and progesterone as oral contraceptive for inhibition of hypothalamic pituitary hormones and suppression of ovulation. • Progesterone potentiate the inhibitory effect of oestrogen on LH secretion.
Adverse effects of administered oestrogen (oral contraceptive). • Water and salt retention. • Effects on blood clotting (↑ risk of thromboembolism because oestrogen ↑ the synthesis of clotting factors and it change the platelet adhesiveness). • Biochemical disturbances, oestrogen ↑ the level of circulating plasma globulin which bind iron, cortisol and thyroxine ↑ their plasma levels, it disturbs CHO metabolism ↓ tolerance to glucose.
Progesterone • Natural progesterone mainly synthesized in the corpus luteum (by theca lutein cells of the follicle). • Large amount of progesterone produced by the placenta during pregnancy. • Also it is found as an intermediary product in steroid hormone synthesis. • It is carried in the blood bound to plasma proteins and it metabolized in the liver and excreted in urine.
Actions • To induce secretory changes in the oestrogen primed endometrium during the luteal phase of the menstrual cycle (changes necessary for implantation). Also secretory changes in the fallopian tubes which provides nutrition for the ovum. • It exerts an anti-oestrogen effect on the endometrium by ↓ the oestrogen receptors and by ↑ the rate of conversion of 17B oestradiol to oestrogen with weaker physiological effects. • It exerts anti-oestrogen effects on the myometrium making it less excitable and less sensitive to oxytocin.
In the breast development, it exerts its effect on the alveolar tissue and lobules in growth in size during adolescence and pregnancy. • During pregnancy, it plays a role in the maintenance of pregnancy by inhibiting uterine muscle activity (relaxing effect). • It prepares the mammary glands for lactation together with oestrogen. • It exerts thermogenic effect which causes raised BMR during pregnancy. • It stimulate the respiratory center causing hyperventilation and ↓ arterial PCO2.
The menstrual cycle • Monthly cyclic physiological events which prepares the female for pregnancy, the cycle ends in menstruation if pregnancy doesn’t occur. • The duration of the cycle is 28 days from the onset of menses to the next with a range of 21-35 days.
The ovarian cycle Each month a few primordial follicles start to grow in response to the rising level of pituitary FSH. Most of the follicles will undergo atresia and only one “leading” follicle will continue development and be able to respond to LH and progress to ovulation. The functional and morphological changes which occur in the ovaries and ovarian follicles during menstrual cycle divided into 3 stages:
1) Follicular development • Involves changes in 3 components of the primordial follicles, the oocyte, the granulosa cells and the theca cell layers. • The granulosa cells proliferate to form several layers with fluid spaces between cells which join to form a single fluid filled space or antrum. The granulosa cells respond to FSH by synthesizing oestrogen. • The oocyte enlarges and becomes surrounded by azonapollucida, mucopolysaccharide layer or some layers of granulosa cells known as the cumulus oophorus.
The theca cells differentiate into a well vascularized theca interna and less vacularized theca externa. The theca cells respond to LH by synthesizing androgens which pass the granulosa cells to be transformed into progesterone. • During the follicular phase the rising level of oestrogen exerts a negative feedback on FSH secretion. The increase in oestrogen and towards the mid-cycle with ↑ the sensitivity of the pituitary to GnRH exerts positive feedback on LH and FSH causing mid-cycle peak of LH.
2) The ovulatory process • It occurs about 24-36 hours following LH peak between the 12th and 15th days of a 28 day cycle.
3) The luteal phase • After ovulation the follicle becomes the corpus luteum and secretes both oestrogen and progesterone. As the level of these 2 hormones ↑ they inhibit the secretion of GnH by negative feedback. If no pregnancy, there is gradual atrophy of the corpus luteum and decline in oestrogen and progesterone which will remove the negative feedback effect from the pituitary leading to premenstrual rise of FSH maturation of more follicle for the next cycle.
The uterine cycle – the myometrial and endometrial tissues respond to the ovarian hormones
The myometrium • Oestrogen increases the uterine blood flow. • The increase in oestrogen and progesterone decreases the myometrial activity. To ↓ uterine muscular activity at mid-cycle and early luteal phase for implantation.
Endometrial changes Within 48 hours after the menstruation, there is change in the epithelial layer from the remnants of glands in the basal part of the endometrium and it responds to ovarian hormones. There are 3 phase; proliferative phase, secretory phase and menstrual phase
a) The proliferative phase – it starts from the end of menstruation and lasts until the time of ovulation. The glands appear tubular, lined by low columnar cells, they become large and convoluted. The stromal cells ↑ in number and become more oedematous. The blood supply also grows. The basal layer supplied by straight arteries and the superfacial part is supplied by spiral arteries (endometrium grows from 0.5mm to 5mm). Oestrogen is the dominant hormone and it corresponds to the follicular phase of the ovary.
b) The secretory phase – from the time of ovulation until menstruation, progesterone is the dominant hormone and it corresponds to the luteal phase of the ovary, under the influence of progesterone endometrial growth ceases and there is functional changes to prepare the tissue for the embryo. The glands start to secrete and discharge their contents into the lumen of the glands (which consists of glycogen, sugars, acids, mucus and enzymes such as alkaline phosphatase). The arteries become more prominent and more coiled and continue to grow while the endometrium height remains static. In the late luteal phase changes depends whether implantation has taken place or not
Implantation – if pregnancy occurs, the developing embryo secretes hCG which maintains the corpus luteum which continue to secrete oestrogen and progesterone. Changes in the endometrium occurs and involve the stromal cells which differentiate into 3 layers • Non-implantation – in the absence of hCG, the corpus luteum decline and falls in both oestrogen and progesterone. There is reduction in the endometrium tissue height and more coiling of the spiral arteries stasis, ischaemia and blanching of the endometrium, local release of prostaglandin causes rhythmic contractions in the spiral arteries
c) Menstruation – interstitial haemorrhages due to breakdown of the superficial arteries and non viable tissues are extended into the uterine cavity and lead to menstrual flow. There is shedding of all the layers except the deep endometrial layer.