Download
1 / 77
790 likes | 845 Views
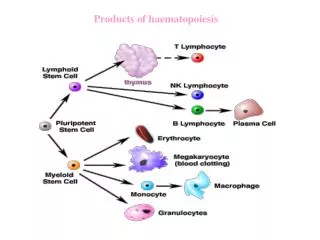
Explore the highly organized differentiation process of haematopoiesis, from embryonic development to bone marrow function. Learn about the role of haematopoietic stem cells and the importance of BONES as haematopoietic organs.

E N D
Haematopoiesis • aka haemopoiesis • and nb if US spelling, hemo-
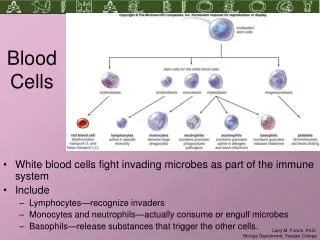
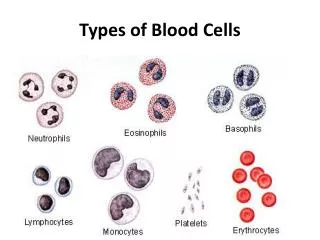
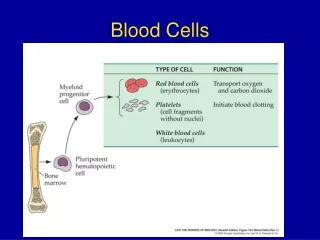
Haematopoiesis • This is the process by which ALL blood cells (= haematological system) are produced • platelets, red blood cells, leukocytes of all sorts • (AND probably also endothelium).
Haematopoiesis • Haematopoiesis is a highly organised differentiation process involving the ordered expression of different sets of genes • It is controlled by factors in the environment of the developing blood cell – the bone marrow in adults • just like any other developmental programme.
The haematopoietic stem cell • Mature blood cells in healthy individuals mostly have short lifetimes (exception: lymphocytes) and are constantly regenerated in the bone marrow. • we make 5 x 1011 blood cells daily • This is accelerated when there is haematological stress • e.g. infection, need more leukocytes • e.g. high altitude, need more red cells.
Haematopoiesis • Haematopoiesis begins at a very early stage in embryonic development, at about 3 weeks in the human. • At that time the cells in the embryo separate into 2 sets, one generating the embryo proper & all the tissues of the adult, the other forming the YOLK SAC (aka vitelline sac) which is the site where blood cells and blood vessels are first formed.
Haematopoiesis • The yolk sac is an ovoid structure joined to the embryo by a stalk. • It contains mesoderm derived cells • “haemangioblasts” • which differentiate to form (nucleated) red blood cells and endothelial cells which generate a capillary system (“plexus”) within the yolk sac.
Haematopoiesis • At the same time the heart and aorta start to form: these join up with the capillary plexus and the erythrocytes start to circulate.
Human foetus about 5 weeks gestation YS = yolk sac Ao = aorta Square = location of limb bud
Haematopoiesis • At a later stage of embryogenesis (after about week 6 in humans) haematopoiesis occurs mainly in the liver and at birth shifts to the bone marrow (BM). • This haematopoiesis is described as definitive unlike the early primitive haematopoiesis occurring in the yolk sac. • Now, the entire range of blood cells found in the adult are produced.
Haematopoiesis • The BM is in effect a highly specialised tissue comprising a range of cells • some of which (haematopoietic cells) form blood cells • others (stromal cells) provide a support functions for the haematopoietic cells, providing the specialised environment needed for haematopoiesis to occur. • Yet other cells (osteoblasts and osteoclasts) are concerned with producing the bone itself.
Haematopoiesis (Bear in mind that cells of the immune system undergo further proliferation and differentiation in the periphery – especially in secondary lymphoid tissue – during immune responses: the purpose of haematopoiesis is to generate cells which are capable of responding to pathogens.)
dem bones – more than a framework to hang muscles from
bones • Source of skeletal rigidity • reservoir of Ca2+ and PO43- • haematopoietic organs.
bones • Bone is a specialised form of connective tissue (mesodermal/mesenchymal origin) with an extracellular matrix (ECM) which is rigid http://www.emedicine.com/orthoped/TOPIC403.HTM • Rigid outer layer of dense compact (aka cortical)bone, 70% hydroxyapatite (hydrated calcium phosphate) • Inner core of much less dense spongy bone (aka cancellous, trabecular).
Long bone (location of BM)
Schematic of cross section of long bone contains blood vessels nerves and lymphatics joins together Haversian canals http://en.wikipedia.org/wiki/Bone The osteon is the unit structure of compact bone made up of concentric mineralised lamellae around a central (Haversian) canal.
Histological section of compact bone showing Haversian and Volkman’s canals.
bones • The bone marrow (BM) is within the medullary cavity especially of long bones. • As mentioned it is intensely cellular because that is where blood cells are produced.
Histological section of bone marrow blood vessels bone trabeculae trabecula = strand (here, of bone)
bones • Bones always start (in development) from cartilage: this is converted to bone by deposition of hydroxyapatite (a form of calcium phosphate) by osteoblasts. • But throughout life, bone tissue is renewed • this is due to a balance between degradation due to osteoclasts and production due to osteoblasts.
bones • Osteoblasts (a type of BM stromal cell) are responsible for laying down a collagen matrix (osteoid) & they subsequently mineralise this with hydroxyapatite. • They are activated by growth factors e.g. bone morphogenic protein (BMP) & certain steroid hormones e.g. oestrogens.
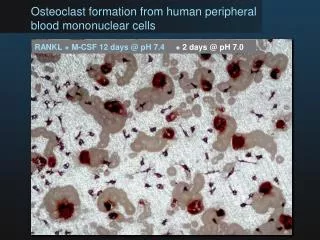
bones • Osteoclasts (derived from haematopoietic cells) resorb bone. • They are activated by certain cytokines e.g. IL-6. • They secrete acids which dissolve the hydroxyapatite and proteases which degrade the collagen.
bones • This balance between production and degradation can be disturbed in some diseases where the osteoclasts get the upper hand • e.g. osteoporosis due to low levels of oestrogen, myeloma due to high levels of IL-6.
Osteolytic lesions in a case of myeloma.
The haematopoietic stem cell • Haematopoietic stem cells (HSCs) are the parental cell type for ALL blood cells • and probably also endothelium. • HSCs are (usually) present only in the bone marrow • also present in cord blood and in (adult) peripheral blood after treatment with “mobilising” cytokines.
The haematopoietic stem cell • The HSC is (probably) able to divide indefinitely, or at least a very large number of times • experiments in 1960s in which mice were irradiated or treated with drugs to destroy their bone marrow showed that transplantation of very small numbers of bone marrow (BM) cells could “reconstitute” the mouse • serial transplant could be done.
The haematopoietic stem cell • Experiments in the 1970s showed that all blood cell types could be derived from single BM cells.
The haematopoietic stem cell • These depended on irradiating the BM cells used to reconstitute the mice with SMALL doses of radiation, not enough to kill the cells but enough to cause minor chromosome alterations (“chromosomal markers”) in rare cells • each marker unique; • all descendents of a marked cell (a CLONE) have the same maker.
The haematopoietic stem cell • In some individual transplanted mice there could be found cells of all leukocyte types bearing the same marker • hence a singlepluripotent stem cell present in the transplant was capable of giving rise to all lineages. • (Probably not totipotent i.e. cannot make all body cells.)
The haematopoietic stem cell • In other mice, ALL myeloid but NOT lymphoid cells had the same marker • And in yet others ALL lymphoid but NOT myeloid cells had the same marker.
The haematopoietic stem cell • This implied that there were also stem cells of more restricted potency • capable of producing EITHER myeloid OR lymphoid cells • these are now known as common lymphoid or myeloid progenitor cells • CLP & CMP.
CLP (common lymphoid progenitor) Lymphocytes HSC Granulocytes erythrocytes thrombocytes CMP (common myeloid progenitor) The haematopoietic stem cell • Hence:
The haematopoietic stem cell • Stem cell self renewal: • evidently since mature leukocytes die the HSC must be able to proliferate at least over the lifetime of the individual. • This proliferation must be assymetric to generate a progenitor cell (CMP or CLP) which has more limited differentiation capacity AND replace the stem cell.
The haematopoietic stem cell • CMPs and CLPs are transient amplifying (TA) cells & proliferate PRIOR TO further differentiation (i.e. before they become granulocytes or whatever) • this is a limited proliferation, increasing cell numbers.
HSC The haematopoietic stem cell CMP CMP proliferation of progenitors to amplify numbers CMP CMP CMP CMP CMP CMP CMP (or CLP) CMP CMP CMP asymmetric division to generate progenitor cell & replace HSC
The haematopoietic stem cell • What is the HSC? • A rare (<0.1%) cell present in bone marrow expressing the antigen CD34. • We now know that CD34+ cells are the essential cell type for BONE MARROW TRANSPLANTATION. • Other cells express CD34 (e.g. endothelial cells) so it us not a unique marker for HSCs.
The haematopoietic stem cell • It is argued that stem cells require a specialised environment to maintain the “stem-ness” of the stem cell: • the stem cell niche. • HSCs are found in two locations in BM: • the endosteum (boundary between solid bone & marrow) associated with osteoblasts; • the perivascular region around vascular sinusoids (large blood vessels with thin-walled comprised of fenestrated endothelium).
The haematopoietic stem cell • Hence “endosteal” and “vascular” niches. • Do they have different roles? • It has been suggested that the endosteal niche contains long-term, slowly dividing HSCs which maintain the vascular niche HSCs. • In the vascular niche the HSCs are more actively dividing and progenitor cells are produced.
HSC niches in the BM endosteal niche vascular niche osteoblast endothelium sinus CMP CMP HSC HSC CLP endosteum
The haematopoietic stem cell • It is not clear what molecules are involved in defining the stem cell niches • presumably adhesion molecules & diffusible factors produced by the non-HSC (“stromal”) cells – osteoblasts, endothelial cells etc – within the niche.
Li, Z. & Li, L. (2008) Understanding hematopoietic stem-cell microenvironments. Trends in Biochemical Sciences 31:589-505 Say no more
growth and differentiation • As the HSC divides, one cell leaves the niche and becomes a progenitor cell, the other stays put • asymmetric division in space as well as in kind niche containing stem cell niche containing dividing stem cell niche containing stem cell and progenitor cell outside niche
growth and differentiation • Evidently the progenitor cell is now in a different environment. • Growth factors drive its growth and then differentiation. • (Perhaps the job of the stem cell niche is to slow cell division and block differentiation.) • The different phases of differentiation and the growth factors required have been largely worked out by cell culture experiments.
growth and differentiation • In vitro culture of bone marrow cells • culture of BM cells is often done suspended in semi-solid media so that the progeny of a single cell can be seen as a colony.
Haematopoietic colonies in semi-solid medium other blood cells erythrocytes