Download
1 / 36
360 likes | 457 Views
Strengthening the weakest link in the chain of survival - CPR in circulation, coronary perfusion, and defibrillation support is critical. Challenges include quality, interruptions, hyperventilation, and perfusion. Studies reveal the impact of interruptions, compression depth, and hands-off intervals on CPR effectiveness.

E N D
The Chain is as strong as the weakest link…. So identifying and strengthening this link is of utmost importance
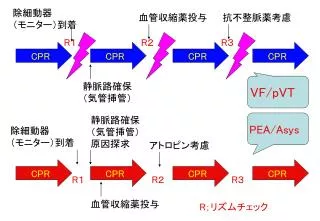
Circulation is Critical for Survival • Provides oxygen to preserve vital organ function • Converts non-shockable rhythms (asystole, PEA) to shockable ones (VF, VT) • More than half of all arrests involve non-shockable rhythms
Presenting Rhythms in SCA Recent studies show that VF or VT is the initial rhythm less than 50% of the time Peberdy MA et al. Resuscitation. 2003;58:297-308. Kaye W et al. JAMA. 2002:39(5),Suppl A. Cobb L et al. JAMA. 2002;288(23):3008-3013.
Coronary Perfusion and ROSC A well perfused myocardium is more likely to experience return of spontaneous circulation (ROSC)
CPP and ROSC (Paradis et al.) Victims with CPP < 15 mmHg do not achieve ROSC With conventional CPR, the overall mean CPP = 12.5 Paradis NA et al. JAMA. 1990;263:1106-1113.
AHA/ERC Guidelines 2005: CPR “Simply put: …push hard, push fast, allow full chest recoil, minimize interruptions in compressions…” Circulation. 2005;112:IV-206.
ERC Guidelines 2005: CPR • High quality, consistent and uninterrupted chest compressions • Push hard, push fast • Compression to ventilation ratio: 30:2 • Rate: 100 manual compressions per minute • Depth: 4 - 5 centimeters • Duty cycle: 50% - 50% • Ventilation: 8 -10 breaths per minute
CPR Challenges • Poor quality • Inconsistent rate, depth, duty cycle • Harmful interruptions • Required due to clinician fatigue, patient transport • Inadequate cerebral and coronary perfusion • Ineffective defibrillation support
CPR Challenges: Quality (Abella et al.) • “…quality of multiple parameters of CPR was inconsistent and often did not meet published guideline recommendations….” Abella BS et al. JAMA. 2005;293:305-310.
CPR Challenges: Quality (Abella et al.) Rate too slow Depth too shallow Ventilation rate too high Abella BS et al. JAMA. 2005;293:305-310.
CPR Challenges: Quality (Wik et al.) “…chest compressions were not delivered half of the time, and most compressions were too shallow…” Flow No Flow • Wik L et al. JAMA. 2005;23 299-304.
CPR Challenges: Interruptions (Kern et al.) “…Any technique that minimizes lengthy interruptions of chest compressions during the first 10 to 15 minutes of basic life support should be given serious consideration in future efforts to improve outcome results from cardiac arrest….” Flow No Flow • Kern KB et al. Circulation. 2002;105:645-649.
CPR Challenges: Hyperventilation Hyperventilation induces hypotension Mean ventilation rate: 30/minute ± 3.2 16 seconds v v v v v v v v v v first group: 37/minute ± 4 after retraining: 22/minute ± 3 Aufderheide TP et al. Circulation. 2004;109:1960-1965.
CPR Challenges: Perfusion (Kern) Manual CPR provides minimal blood flow to the heart and brain 10% - 20% of normal flow 30% - 40% of normal flow Kern KB Bailliere’s Clinical Anaesthesiology. 2000;14(3):591-609.
CPR Challenges: Interruptions (Edelson, Abella et al.) 77% decrease in ROSC when pre-shock time increased from </= 9.7 seconds to </= 22.5 seconds • Edelson et al. Circulation. 2005;112(17)II-1099 Edelson DP, Abella BS et al. Circulation. 2005;112(17):II-1099.
CPR Challenges: Interruptions (Berg et al.) Interrupting chest compressions for rescue breathing can adversely affect hemodynamics during CPR for VF Blood pressure Berg et al, 2001 Time Chest compressions Berg RA et al. Resuscitation. 2001;104:2465-2470.
CPR Challenges: Defibrillation Support After ~4 minutes of VF, the myocardium is nearly depleted of ATP*, a vital energy source needed for successful defibrillation *Adenosine triphosphate (ATP), which breaks down into adenosine diphosphate (ADP).
Myocardial Cell<10% ATP Myocardial Cell30-40% ATP Myocardial Cell100% ATP
CPR Challenges: Defibrillation Support Effective compressions help restore ATP, increasing the likelihood of successful defibrillation
100% P<0.01 P<0.01 88% 60% 50% Compression Depth and Shock Success Edelson et al. Resuscitation 2006 Nov ;71(2):137-45
60 consecutive VF arrests at U Chicago Shock success after 1st DF 94% 72% 60% 38% Hands-Off Interval vs Shock Success Edelson et al. Resuscitation 2006 Nov ;71(2):137-45
Conclusions The quality of CPR prior to defibrillation directly affects clinical outcomes. Specifically, longer pre-shock pauses and shallow chest compressions are associated with defibrillation failure. Strategies to correct these deficiencies should be developed and consideration should be made to replacing current-generation automated external defibrillators that require long pre-shock pauses for rhythm analysis. Edelson et al. Resuscitation 2006 Nov ;71(2):137-45
Abella BS, Kim S, Edelson DP, Huang KN, Merchant RM, Myklebust H, Vanden Hoek TL, Becker LB. Difficulty of cardiac arrest rhythm identification does not correlate with length of chest compression pause before defibrillation. Crit Care Medicine2006 Dec; 34(12 Suppl):S427-31
Design • Prospective in-hospital study of cardiac arrest resuscitation attempts coupled with a retrospective review of preshock pause rhythms by 12 trained providers. Reviewers scored rhythms by ease of identification using a discrete Likert scale from 1 (most difficult to identify) to 5 (easiest to identify). The resuscitation cohort was organized into preshock pause-duration quartiles for statistical analysis. Resident physicians were then surveyed regarding human factors affecting preshock pauses.
Results • A total of 118 preshock pauses from 45 resuscitation episodes were collected. When evaluated by quartiles of preshock pause duration, difficulty of rhythm identification did not correlate with increasing pause time. • In fact, the opposite was found (longest preshock pause quartile of 23.8-60.2 secs vs. shortest pause quartile of 1.1-7.9 secs; rhythm difficulty scores, 3.2 vs. 3.0; p = .20). • When 29 resident physicians who recently served on resuscitation teams were surveyed, 18 of 29 (62.1%) attributed long pauses to lack of time sense during resuscitation, and 16 of 29 (55.2%) thought that room crowding prevented rapid defibrillation.
Conclusion • Long cardiopulmonary resuscitation pauses before defibrillation are likely due to human factors during the resuscitation and not due to inherent difficulties with rhythm identification. This preliminary work highlights the need for more research and training in the area of team performance and human factors during resuscitation.
Gavin D. Perkins, William Boyle, Hannah Bridgestock, Sarah Davies, Zoe Oliver, Sandra Bradburn, Clare Green, Robin P. Davies, Matthew W. Cooke Quality of CPR during advanced resuscitation training Resuscitation volume 77 issue 1 pages 69-74 ( April 2008 )
Design • Observational study of quality of CPR during advanced life support training courses before and after the implementation of the European Resuscitation Council Guidelines 2005 into the ALS course. The quality of chest compressions were downloaded from a manikin and direct observations of no-flow time; pre-shock pauses were recorded.
Results • 94 cardiac arrest simulations were studied (46 before implementation of Guidelines 2005 and 48 after). • Delays in starting CPR, inadequate compression depth, prolonged interruptions of chest compressions and excessive pre-shock pauses were identified. • The introduction of Guidelines 2005 resulted in improvements in the number of compressions given per minute and a reduction in no-flow time and duration of pre-shock pauses • overall the quality of CPR performed during the ALS course remained poor. • There was little evidence of performance improving over successive simulations as the course progressed.
Conclusion • The implementation of Guidelines 2005 into the ALS course appear to have improved the process of CPR by reducing no-flow time during simulated CPR. However, the quality of CPR during ALS training remains sub-optimal. Delays in starting CPR, inadequate compression depth, excessive interruptions in chest compressions and prolonged pre-shock pauses mirror observations from clinical practice. Strategies to improve CPR performance during ALS training should be explored and potentially may result in improvements in clinical practice.
Current handposition • The current approach to chest compressions • In 80% of the 189 patients’ CT images, the intrathoracic structure just underneath the INL was the ascending aorta (18.0%), the root of aorta (48.7%), or the left ventricular outflow tract (12.7%), rather than the left ventricle itself • Jungho, Joong and Kyuse, Resuscitation (2007) 75, 305—310
Current handposition For more efficient and effective chest compression during CPR, compressing the sternum more caudally than the INL should be considered if it is not associated with the risk of increasing internal visceral injuries Jungho, Joong and Kyuse, Resuscitation (2007) 75, 305—310
Resuscitation (2008) 79, 1—3 Defibrillation—–Safety versus efficacy Gavin D. Perkins, Andrew S. Lockey