Download

1 / 29
300 likes | 551 Views
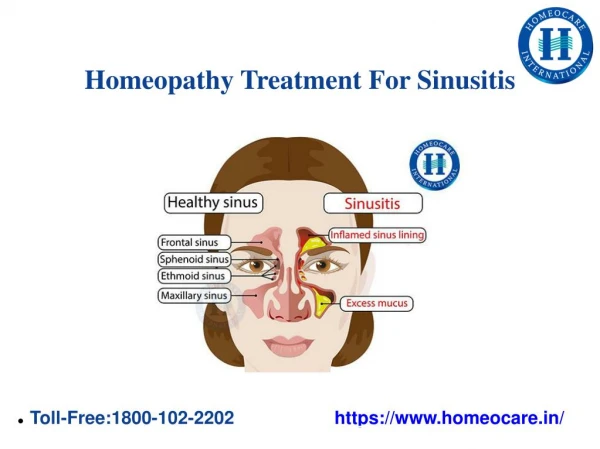
Osteopathic Treatment For Patients With Sinusitis. 3D frontal view. 47 Year old female with frontal headache and yellow nasal discharge. Fronto-occipital headache, face pain and sore throat x 4 days Unable to clear secretions when blowing nose Post nasal drip with minimally productive cough

E N D
47 Year old female with frontal headache and yellow nasal discharge • Fronto-occipital headache, face pain and sore throat x 4 days • Unable to clear secretions when blowing nose • Post nasal drip with minimally productive cough • Gets 2-3 sinus infections/year
PM/Surg/Soc/FamHX: • Occipital/Tension headaches • GERD, usually controlled but symptomatic when has post nasal drip • Irregular menses/perimenopausal • Environmental allergies trigger sinusitis in spring and fall • sinus surgery 2 yrs ago helped, but didn’t resolve problems • Nonsmoker, no pets • Several siblings with chronic sinus problems
Trauma/Birth History • Onset occipital headaches when stood up into a 4x6 board 12 years ago, hitting on the back of the head. Lost consciousness for a few minutes. • Was a “large baby”, otherwise unknown
Meds/Allergies • Omeprazole, Loratidine, Multivitamin, Calcium +D. • Azithromycin, Guaifenesin, nasal steroids are the usual sinusitis regimen that resolves her symptoms • NKDA
VSS Afebrile NAD HEENT: NC/AT, face symmetrical TM grey with good landmarks but left retracted. No effusion. Nasal mucosa swollen with yellow drainage from ostia L Pharynx injected, pebbled, without exudate or tonsillar enlargement Yellow post-nasal drip Physical Exam
Physical Exam • Tender to palpation frontal, nasal and left maxilla • No cervical, supraclavicular or infraclavicular adenopathy • Lungs CTAB • Heart RRR without murmur • Minimal epigastric tenderness, no mass/rebound tenderness/rigidity/guarding
0 Structural Exam • Thoracic inlet sidebent right, rotated left • First rib superior on the left • Positive Left anterior subclavicular Chapman’s reflexes • Bilateral posterior upper cervical Chapman’s reflexes • C2 FRSR • OA FSLRR
More Structural Exam • Decreased CRI • Poor compliance/tender at left mastoid process and nasion • Left maxilla internally rotated • Left pterygopalatine fossa soft tissues boggy
0 Possible treatment sequence for this patient • Indirect or direct MFR to thoracic inlet and thoracoabdominal diaphragm if needed • ME, FPR or BLT to left first rib • Treat posterior cervical Chapman’s reflexes. • Check to see if anterior reflexes less tender. If not, treat them too. • Treat upper cervicals with suboccipital release, ME, BLT or Still • Sacral motion restriction may need to be addressed.
Sympathetic Relationships in the Cervical Region: Superior cervical ganglion Middle cervical ganglion Inferior cervical ganglion
0 Where would you start for this set of cranial findings? • Decreased CRI • Poor compliance/tender at left mastoid process and nasion • Left maxilla internally rotated • Left pterygopalatine fossa soft tissues boggy
Possible sinusitis techniques • Choose which apply to your site then delete the irrelevant slide(s) • Venous sinus drainage sequence (precede with OA release and end with frontal/parietal lifts) • Fronto-zygomatic lift • Alternating lateral rocking of the nasion • Sphenopalatine ganglion release • Percusssion/ “jello tap” over involved sinuses • Effleurage over frontals, nasals, maxillae and towards mastoids • Supra & Infra orbital nerve stimulation
Cephalad Hand contacts the frontal with two finger pads Caudad Hand contacts the two nasal bones with thumb and index Gently distract Can also be done for fronto-maxillary sutures. Fronto-nasal Release
Supraorbital and Infraorbital Foramina • Locate the foramen along the superior orbital ridge or the inferior orbit • Gentle finger pad contact is used to massage the nerve and surrounding tissues • A slow rotary motion back and forth is often quite effective. • This can be easily taught to the patient for home use.
Sphenopalatine Ganglion Intimate relationship with the Maxillary Branch of the Trigeminal N. • Note Relative flatness of pterygoid process compared to rounded maxilla Sutherland, Teachings in the Science of Osteopathy, p. 96
Sphenopalatine Ganglion • Note that the spenopalatine ganglion is suspended from the maxillary nerve Sutherland, Teachings in the Science of Osteopathy, p. 96
Treatment of the Sphenopalatine Ganglion • Stand opposite the side to be treated • Caudal Hand: Introduce the little finger of the caudal hand softly & carefully along the alveolar ridge past the tuberosity of the maxilla on to the lateral plate of the pterygoid – it is a flatness in contrast to the curved maxilla • The patient may have to move the ramus of the jaw laterally to create room for the finger Craniosacrale Osteopathie II, p.99
Treatment of the Sphenopalatine Ganglion • Once in position have the patient tip the head against the pad of the little finger to tolerance, or • apply gentle inhibitory pressure medially & cranially in the direction of the outer orbit • It can be quite painful • Pressure on the ganglion will stimulate it to action which will be indicated by lacrimation • Decreased tissue tension also indicates completion of this technique Craniosacrale Osteopathie II, p.99
References • Grant’s Atlas Digital Images • American Academy of Otolaryngology - Head and Neck Surgery One Prince StreetAlexandria, VA 22314-3357 • http://www.entnet.org/healthinfo/sinus/sinus_side.cfm
Treatment of the Sphenopalatine Ganglion • Fluid-wave Technique: • Cranial Hand’sThumb is on the coronal sutureopposite the sphenopalatine ganglion contact – at the longest diameter • Gentle pressure is directed toward the ganglion in coordination with the cranial impulse • Unwinding Technique: • Cranial Hand contact on the greater wings to monitor motion • Release will follow from a forceful flexion motion that can be felt By the cranial hand Craniosacrale Osteopathie II, p.99
Facilitators • Do not try to go through the venous sinus drainage technique during the presentation. It takes too long • Students can be given a handout of it to take home for practice.