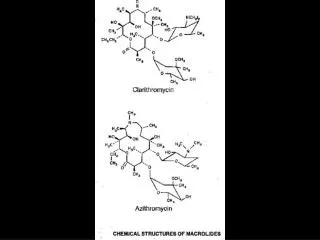
NEWER MACROLIDES
NEWER MACROLIDES. Improved acid stability, tissue penetration. Broader spectrum of activity. ANTIMICROBIAL ACTIVITY. Most active against gram-positive cocci and bacilli. Mycoplasma , Legionella and Chlamydia. ANTIMICROBIAL ACTIVITY. Mycobacterium avium intracellulare (MAC). ABSORPTION.

NEWER MACROLIDES
E N D
Presentation Transcript
NEWER MACROLIDES • Improved acid stability, tissue penetration. • Broader spectrum of activity.
ANTIMICROBIAL ACTIVITY • Most active against gram-positive cocci and bacilli. • Mycoplasma, Legionella and Chlamydia.
ANTIMICROBIAL ACTIVITY • Mycobacterium avium intracellulare (MAC).
ABSORPTION • Macrolides are incompletely but adequately absorbed from the GI tract. • Erythromycin base is inactivated by stomach acid. • Made in various acid resistant forms. • Food interferes with absorption.
ABSORPTION • Erythromycin estolate is absorbed best. • Usually no one preparation offers a significant therapeutic advantage. • The newer macrolides are absorbed more rapidly than erythromycin.
DISTRIBUTION • Well distributed except into the CNS. • In meningitis enough gets into the CNS to be therapeutically effective.
METABOLISM AND EXCRETION • Most of the erythromycin is metabolized. • Erythromycin is concentrated in the liver and excreted in active form in the bile.
THERAPEUTIC USES • A useful alternative to the penicillins. • Infections caused by pneumococci and group A streptococci with penicillin allergy. • Minor infections caused by penicillin resistant or sensitive Staph. Aureus. • Prophylaxis of rheumatic fever and subacute bacterial endocarditis.
MYCOPLASMA PNEUMONIA • A macrolide or tetracycline is the drug of choice for Mycoplasma infections. • Reduces the duration of fever and accelerates the clearing of the chest radiographs.
CONTRAINDICATIONS • Pregnancy (the estolate)-because of the possibility of hepatotoxicity. • Hepatic dysfunction.
DRUG-DRUG INTERACTIONS • Erythromycin (and clarithromycin) inhibit Cytochrome P-450 enzymes.
Demethylase Erythromycin CytP3A4 Antifungals,verapamil, diltiazem
DRUG-DRUG INTERACTIONS • Drugs that prolong QT interval.
KETOLIDES (Telithromycin) • Unique structure compared to macrolides, allowing it to be used in resistant respiratory infections. • Differs from erythromycin by substitution of a 3-keto group for the neutral sugar L-cladinose.
ANTIBACTERIAL SPECTRUM • Similar antibacterial spectrum to erythromycin but many macrolide-resistant strains are susceptible to ketolides.
THERAPEUTIC USES • Respiratory tract infections, including community acquired bacterial pneumonia, acute exacerbations of chronic bronchitis, sinusitis and streptococcal-pharyngitis.
CLINDAMYCIN • A lincosamide closely related to lincomycin.
ANTIBACTERIAL ACTIVITY • Similar to erythromycin. • Anaerobic bacteria, especially Bacteroides.
PHARMACOKINETICS • Absorbed rapidly and nearly completely following oral administration. • Widely distributed throughout the body except for the CNS.
Clindamycin Enterohepatic circulation
OXAZOLIDINONES • New class of synthetic antibacterial agents. • Inhibit protein synthesis by a unique mechanism.
LINEZOLID (Zyvox) • The first and one of 2 oxazolidinones presently available.
ANTIBACTERIAL ACTIVITY • Wide spectrum of activity vs. gram positive organisms including methicillin-resistant staphylococci, penicillin resistant pneumococci and vancomycin resistant Enterococcus faecalis and E.faecium. • Several anaerobic organisms.
PHARMACOKINETICS • Good oral bioavailability (also given IV). • Metabolized. • No dosage adjustment necessary with impaired renal or hepatic function.
THERAPEUTIC USES • MRSA. • Vancomycin resistant E.faecium.
Vancomycin resistant enterococcal infections (VRE) • Disproportionately affects patients in the ICU, immunosuppressed hosts, particularly liver and other solid organ recipients and patients with post chemotherapy neutropenia, and patients with intravascular and bladder catheter devices.
VRE • Emerged during 1990’s • Enterococci already possess intrinsic and acquired resistance to most other antimicrobials (β-lactams, aminoglys, lincosamides and cotrimoxazole).
TREATMENT OF VRE • Approved-linezolid and quinopristin/dalfopristin • Available agents which don’t have a specific VRE approval (chloramphenicol, doxycycline, high-dose amoxicillin/sulbactam)
PRECAUTIONS Linezolid Tyramine MAO SSRI toxicity Serotonin Linezolid
Quinupristin/Dalfopristin (Synercid) • First streptogramin to be approved in the U.S. • Present in a ratio of 30:70.
ANTIBACTERIAL ACTIVITY • Bactericidal vs. susceptible strains of staphylococci and streptococci. • Bacteriostatic vs. Enterococci faecium.
ANTIBACTERIAL ACTIVITY • Active vs. a wide range of gram positive bacteria including staphylococci resistant to methicillin, quinolones and vancomycin; pneumococci resistant to penicillin and E.faecium strains resistant to vancomycin.
PHARMACOKINETICS • Administered IV (over 1 hr).
THERAPEUTIC USES • Vancomycin strains of E.faecium and complicated skin infections caused by Staph. • Serious infections caused by multiple drug-resistant gram-positive organisms.
DRUG INTERACTIONS • Inhibits cytochrome CYP3A4.
Review-Drugs vs. Gram+ Organisms • Penicillins (G,V and antiStaph) • 1st. Generation Cephs. • Macrolides • Vancomycin • Linezolid • Streptogramins
1.5 Estolate Stearate Erythromycin Base 1.0 Serum Levels mcg/ml 0.5 0.5 1.0 2.0 3.0 4.0 5.0 6.0 7.0 8.0 Hours Serum Concentration After Oral Administration of Different Erythromycin Preparations
VANCOMYCIN • Tricyclic glycopeptide antibiotic. • Antibacterial activity-primarily active against gram positive bacteria.
MECHANISM OF ACTION • Bactericidal. • Inhibits cell wall synthesis (2nd stage of cell wall synthesis). • Binds with high affinity to the D-alanyl-D-alanine terminus of cell wall precursor units, at the crucial site of attachment and thereby inhibits vital peptidoglycan polymerase and transpeptidation reactions.
Glycopeptide Polymrer Mur NAc X Vancomycin X Glycopeptide Polymer Mur NAc X D-Alanine Transpeptidase