Download
1 / 20
510 likes | 2.28k Views
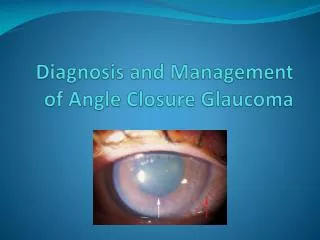
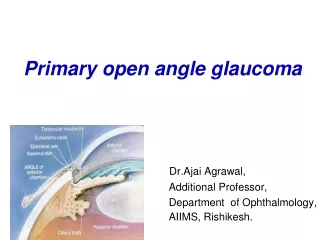
Diagnosis and Management of Angle Closure Glaucoma. Angle Closure Glaucoma (ACG). Introduction Readings: Bartlett & Jaanus, pp. 693-694, Kanski, pp. 421-436 Overview: Risk factors for Narrow Angles Primary Angle Closure Attack Intermittent Angle Closure Primary Angle Closure Suspect

E N D
Angle Closure Glaucoma (ACG) • Introduction • Readings: Bartlett & Jaanus, pp. 693-694, Kanski, pp. 421-436 • Overview: • Risk factors for Narrow Angles • Primary Angle Closure Attack • Intermittent Angle Closure • Primary Angle Closure Suspect • Primary Angle Closure
ACG • Narrow Angles • “anatomical condition in which there is iridotrabecular apposition caused by any number of factors” • TM not visible on gonioscopy in two quadrants (180 degrees) • Incidence about 1% of general population
ACG • Sad Stats • About 1/3 of patients worldwide • 25% blind • 2-3x blinding potential vs OAG (open angle glaucoma)
ACG • Risk Factors • Increasing age • Increasing lens thickness • Phacomorphic component • Relatively anterior lens positions: shallow anterior chamber depth • Female gender • Hyperopia • Ethnicity/Race: Inuit Eskimo, East Asian (Chinese) • Eastern Europeans too, but less common
ACG • Primary Angle Closure Attack • Characterized by quick IOP increase • monocular • Signs and symptoms -usually • Severe eye pain • Conjunctival injection • Tearing • Photophobia • Blur • Halos around lights • Corneal edema • Fixed and dilated pupil • IOP of 50-70 mm Hg: TRUE OCULAR EMERGENCY • Nausea and vomiting
ACG • Primary Angle Closure Attack • Diagnosis • Gonioscopy OU • Vast majority: “pupillary block” mechanism with iridotrabecular apposition in 2 quadrants • Affected or fellow eye has deep angle, a non-pupillary block mechanism is present like Iris Plateau syndrome • Evaluating structures and for peripheral anterior synechiae (PAS)
ACG • Angle Evaluation Via Gonioscopy
ACG • Primary Angle Closure Attack: Causes • Pupillary Block • Closeness of posterior iris to anterior lens • High resistance of forward movement of aqueous through the iris channel • Increased pressure differential between anterior and posterior chambers • iris bombe and angle closure
ACG • Primary Angle Closure Attack: Causes • Choroidal expansion: anterior rotation of the ciliary body with forward movement of iris and lens • No iris bombe • Links: Vogt-Koyanagi-Harada Syndrome syndrome, HIV, cavernous sinus fistula, Panretinal photocoagulation, sulfa-based meds (Topamax, Diamox) • Managed with cycloplegic and steroid • Pilocarpine, Diamox, PI not indicated
ACG • Primary Angle Closure Attack: Causes • Plateau Iris Configuration • Typically in younger patients (< 40 years old) • Anterior ciliary processes pushing up and causing peripheral iris to bow forward • Peripheral iridotomy does not work • Peripheral iridoplasty pushes iris away from the angle • So does pilocarpine, but?
ACG • Primary Angle Closure Attack • Management: Pupillary Block • Oral Carbonic Anhydrase Inhibitor • Diamox (acetazolamide) 500 mg • Contraindications and side effects? • Topical beta-blocker: Timoptic 0.5% • Contraindications and side effects? • Alpha-2 adrenergic agonist: Iopidine • Pilocarpine 2% • Topical steroids • Less commonly used: glycerin (Osmoglyn), IV mannitol
ACG • Primary Angle Closure Attack • Management • Pressure indentation on cornea with gonioscopy lens • Can help “break” the attack • Never used: anterior chamber paracentesis+
ACG • Primary Angle Closure Attack • Management • In-office until IOP < 30 mm Hg • Refer for peripheral laser iridotomy in most cases within 1-2 days • Glaucoma filtration surgery
ACG • Intermittent Angle Closure • Intermittent attacks with spontaneous resolution • With or without symptoms • Over time, result in PAS chronic condition • When? • Pupil in mid-dilated state • Morning, late at night, dim conditions, OTC cold medications (pseudo-epinephrine derivatives), stress • Rx med Topiramate (Topamax)
ACG • Intermittent Angle Closure • Diagnosis • Narrow on Van Herrick gonioscopy • Consider referral for PI (peripheral iridotomy) • Provocative dilation tests • Also called “Subacute Angle Closure”
ACG • Primary Angle Closure Suspect • Diagnosis • Narrow anatomical angles • Normal IOP at exam • Without PAS • Without optic disc damage, intermittent attacks
ACG • Primary Angle Closure Suspect • Management • Depends on gonioscopy results • Grade 01: PI recommended • Grade 12: debatable PI • > grade 2: monitor every 6 months • 2 quadrants (180 degrees) where cannot see TM (trabecular meshwork) refer • “jet-setter” ? • Educate about symptoms, and what to do if they occur • Educate about what puts pupil in mid-dilated state
ACG • Primary Angle Closure Glaucoma • Diagnosis • A chronic condition • Persistent high IOP’s of 20-30 mm Hg • Grade 0-1 angles on gonioscopy with PAS • Check for Plateau Iris Configuration • ONH evaluation or glaucoma work-up • Glaucomatous optic neuropathy and VF loss
ACG • Primary Angle Closure Glaucoma • Management • PI • Medical therapy if IOP still high (PAS) or if combined mechanism