Download

1 / 13
130 likes | 228 Views
Financing Regional Healthcare Katowice, 19-20 th March. Working with the private sector - possibilities offered by Public Private Partnerships Steve Wright European Centre for Health Assets & Architecture. Definition of PPPs.

E N D
Financing Regional HealthcareKatowice, 19-20th March Working with the private sector - possibilities offered by Public Private Partnerships Steve Wright European Centre for Health Assets & Architecture
Definition of PPPs • There are standard definitions, but they don’t recognise the diversity • In essence, there is a spectrum depending on sector, from corporate sponsorship to contractual models • I focus only on latter, & for capital investment: i.e. business models which can achieve replicability, scaleability and durability • Some obvious PPP models – JV companies, concessions, “Private Finance Initiative” • Essentially there are four activities in any capital project – Design, Build, Finance and Maintain: a PPP always has “M” (as well as usually other phases, particularly “F”)
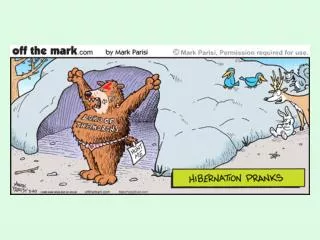
Health (accommodation) PPP Clinical care Contracting hospital authority Ministry of Health Patients Concession contract Equity providers Construction sub-contract Builder Accommodation concessionaire “SPV” Commercial banks or bondholders Lifecycle maintenance: “hard FM” Lifecycle sub-contract Senior loans/bonds & subordinated debt Services sub-contract Catering, cleaning, portering, IT etc: “soft FM”
Traditional public hospital - procurement of an accommodation asset • The public sector or hospital owner: • Prepares a design (i.e. specifies the input) • Raises the budget finance • Selects a builder • The private sector contractor: • Builds the hospital • Gets paid • The public sector or hospital owner: • Owns the hospital • Manages most building services (& medical) • Maintains it (or not)
A PPP hospital – procurement of accommodation services • The public sector or hospital owner: • Prepares a specification of service need (i.e. specifies output) • Selects a partner • [Maintains responsibility for medical aspects] • The private sector contractor: • [Designs the hospital] • Raises the finance • Builds the hospital • Gets paid annually for building services delivered • Maintains the hospital to defined standards • Gets paid annually where standards upheld • Hands the hospital back at the end of the contract
Advantages of PPP… • May provide a solution for capital shortages (but in reality accommodation PPPs are only debt: time-shifting of expenditure) • Helps introduce private sector disciplines in construction & operations • The building is to a higher quality & longer life • Services (not usually the core medical) are handled by dedicated estate experts • Risk is in hands of party best capable of assuming it
Disadvantages of PPP… • Cost of capital is higher for an SPV than a government • Tends to emphasise the big bricks-and-mortar (whereas capital ought to flow to all levels of healthcare) • Potential oligopoly of contractors (high costs of entry – of abortive bidding costs – & of exit) • High commitment transaction costs (lawyers, consultants, bankers…) • High non-contractible operational transaction costs (leads to reduced through-life flexibility for medical services)
Tests of value for money • Is the legal and institutional framework right? • High quality strategic capital planning & option appraisal is essential • Healthcare remains the priority, not method of financing it • Is the public sector team skilled & experienced? • Will the evaluation be robust? • Can they liaise but also negotiate with the contractor? • How is risk to be transferred & to whom? • Simply substituting private for public capital will not give value for money - is risk sharing realistic? • Is there a credible “public sector comparator” (the test for the value of risk transfer)? • Is the scope of the procurement appropriate? • Is there private sector expertise? • Will there be competition?
Contractual models – along a continuum Contract “completeness” (Specification of contingencies in contract) Incomplete Complete Practical PPPs are here Full outsourcing (but only in some “idealised” world) PFI? “Cooperation”? (but not replicable or scaleable…)
Contract “completeness” • Between a provider & its public sector client, absolute contract completeness is in principle desirable: • Certainty for both contracting parties • Appropriate risk transfer • But uncertainty & transaction costs always mean that incompleteness in long-term contracting is inevitable • When there is contract incompleteness, there is an essential trade-off, some part of which will not be contractible: future costefficiency gains versus quality improvement • There still needs to be some control of both parties’ behaviour to avoid opportunism - PPPs are one contracting mechanism, substituting partnership for the desirable but missing contract “completeness” • Rather than over-emphasising comprehensiveness of contract, aim for “contingent adaptability” – get the incentives right for partnership for long-term sustainability
Contract “incompleteness” • When there is contract incompleteness, non-contractible incentives over time on the external providing party are: • Strong to aim for cost reduction, because they are captured by the contractor • Weak to aim for quality improvements (including future flexibility of the estate), because they are given away to public sector • Thus case for in-house (public) provision stronger when: • Cost reductions can seriously damage quality • Quality innovations are unimportant relative to cost issues • Corruption is significant • There are weak unions or weak public patronage Is this a good characterisation of the health sector? If so but you still want a PPP, need to manage it carefully
Conclusions • Capital PPPs are about exchanging purchase of an asset for purchase of ongoing services • There are pros & cons (mainly: transferring responsibility vs later inflexibility) • There are legal, institutional & other pre-conditions to get PPP right • Fruitful to look at PPPs as a contracting mechanism which substitutes partnership for the desirable but inevitably missing contract “completeness” • Incentives for quality versus cost imply trade-offs which need to be managed
Thank you! steve.wright@echaa.eu www.echaa.eu