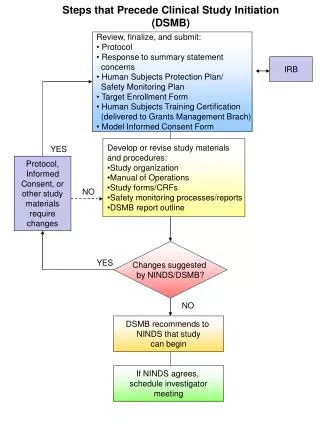
DSMB Experiences
DSMB Experiences. Mary A. Foulkes, Ph.D. Office of Biostatistics and Epidemiology Center for Biologics Evaluation and Research. Association of GCRC Statisticians Toronto August 8, 2004. OPTIMA ERSET ATN ICTDR ACES Hermansky-Pudlak VA Coop Studies. 2002 – Present 2002 - Present

DSMB Experiences
E N D
Presentation Transcript
DSMB Experiences Mary A. Foulkes, Ph.D. Office of Biostatistics and Epidemiology Center for Biologics Evaluation and Research Association of GCRC Statisticians Toronto August 8, 2004
OPTIMA ERSET ATN ICTDR ACES Hermansky-Pudlak VA Coop Studies 2002 – Present 2002 - Present 2002 – 2004 2000 – 2002 1998 – 2004 1998 – 2001 1984 - 1995 DSMB Stat Experience
CHS (OSMB)-NHLBI SOCA – NEI/NIAID Therapeutic Trials Prevention Trials LRC CPPT 1998 – Present NIAID Pgm Rep NIAID Pgm Rep NIAID Pgm Rep 1975 – 1980 Other Experience
OPTIMA HIV+ patients for whom HAART has failed ARDFP + Standard ART NO ARDFP + Standard ART ARDFP + Mega ART NO ARDFP + Mega ART
ERSET Patients with Mesial Temporal Lobe Epilepsy (MTLE), whose seizures have failed to respond to 2 medications, and who have not had disabling seizures for more than 2 years Early surgical intervention Continued optimal pharmacotherapy Primary Outcome: Freedom from disabling seizures Secondary: Freq & severity, QoL, psych & social func
ATN • NICHD Adolescent Medicine Trials Network • HIV+ adolescents • Short-cycle therapy • Structured treatment interruption • Hep-B vaccine trials • QoL, Compliance, VL monitoring
ATN Workload • Two trials -- ~ 4 days/year • Face-to-face – 2 days • Review quarterly reports – ½ day • Conf calls – 1 day • More trials -- ~ 6-7 days/year • Face-to-face – 3 days • Review quarterly reports – 1day • Conf calls – 2 day
ICTDR • Multiple trials in TB, malaria, diarrhea, hantavirus, dengue, malnourishment • Often unblinded, vs stand of care • Multinational enrollment, developing countries • NIAID Div Microbiology & ID network est. 1991
ACES Pts w hx of MI or revascularization or > 50%stenosis Azithromycin 600 mg/wk Placebo 1 tablet/wk
Hermansky-Pudlak Trial Puerto Rican HPS patients w HPS mutations admitted to NIH Clinical Center w FVC 40-75% of predicted Anti-fibrotic (pirfenidone) Placebo
Data Monitoring Committee • Need an Independent DSMB • Mortality or irreversible morbidity outcome • Pivotal Phase III trials • Need independence of stat func www.fda.gov/cber/gdlns/clindatmon.htm
DMC Reviews Recruitment Baseline Variables - Eligibility & Comparability Outcome Measures - Primary & Secondary Toxicity/Adverse Effects Compliance Specified Subgroups
DMC Relationships& Responsibilities • Patients • Study Investigators • Sponsor • Local IRBs • Regulatory Agencies
Early AnalysisDMC and Executive Committee Recruitment/Entry Criteria Baseline Comparisons Design Assumptions • Control only • Combined groups
Design Modifications(For Example) • Entry Criteria • Treatment Dose • Sample Size Adjustment • Frequency of Measurements
DMC Recommendations • Continue Protocol Unmodified • Modify Protocol • Terminate Trial
Reasons for Early Termination • Serious toxicity • Established benefit • Futility or no trend of interest • Design, logistical issues too serious to fix
Decision Philosophy Decide Ahead of Time • Positive Beneficial Trend • How convincing? • Negative Harmful Trend • Symmetric or Asymmetric? • No Trend • Futility?
Complex Decision-making Process • Recruitment Goals • Baseline risk and comparability • Compliance • Primary & secondary outcomes • Safety
Complex Decision-making Process • Internal consistency • External consistency • Benefit/Risk • Current vs. future patients • Clinical/Public impact • Statistical issues
DMC Membership Needed expertise • Clinical • Basic science • Clinical trial methodology • Biostatistics • Epidemiology • Medical ethics • Helpful expertise • Regulatory • Some experience essential
DMC Membership • One can represent multiple areas of expertise • Recommend minimum size of 3 • Max depends on complexity • Recommend size >5 for multicenter trials or multiple trials
DMC Membership • Jointly agreeable to both sponsor and investigators (e.g. Exec Comm) • Formal appointment often made by sponsor or delegated to Exec Comm • An honor but not honorary – must assume serious responsibility
DMC Membership • Groups with conflicts of interest • Sponsor • Industry • Government • Disease Societies • Trial investigators • Regulatory agencies • Individuals with financial incentives or intellectual investment
DMC Chair • A critical appointment • Needs clinical trial experience • Ideally, DMC experience • Consensus building talent
DMC Decision Making Role • DMC makes recommendations, not final decisions • Independent review provides basis for recommendations • DMC makes recommendations to Exec Comm, or to sponsor directly • DMC may, if requested, debrief Exec Comm and/or sponsor • DMC recommendations are rarely rejected
DMC Meeting Format • Open Session • Progress, blinded data • Sponsor, Exec Comm, DMC, SAC • Closed Session • Unblinded data • DMC, SAC • Sponsor rep? (usually not) • Executive Session • DMC only • Debriefing Session • DMC Chair, Sponsor rep, Exec Comm rep
DMC Needs “On-Line”Data Mgmt & Analysis • DMC reluctant to make decisions on “old data” • Be prepared from start (e.g., ACTG 076) • Focus on key variables, not complete case reports (delays can be problematic) • Minimize data delay and event verification (e.g., ACTG 019)
ACTG #019 HIV Progression (8/2/89) 1.00 0.95 0.90 0.85 0.70 Probability ZDV 500 mg Placebo 0 4 8 12 16 20 24 Time to HIV Progression (months)
ACTG #019 HIV Progression (8/16/89) 1.00 0.95 0.90 0.85 0.70 Probability ZDV 500 mg Placebo 0 4 8 12 16 20 24 Time to HIV Progression (months)
Screening & recruitment Baseline variables /Risk factors Compliance Primary & secondary outcomes DMC Report Example: Adverse Events Laboratory outcomes Concomitant therapy Subgroups Interim analysis assessment DMC Report http://www.medsch.wisc.edu/biostat/clintrials/sdac/sdacpdf.html
Masking/Blinding DMC Report • A vs. B, C vs. D, ….. X vs. YNOT RECOMMENDED! • A vs. B for all tables and require masked decisionsNOT RECOMMENDED! • A vs. B for all tables • unblind on a “need-to-know” basis or • identify labels at meetingRECOMMENDED! • Named treatment vs. control tables NOT RECOMMENDED! • DMC masking not an FDA requirement
DMC Confidentiality • In general, interim data must remain confidential • DMC may rarely release specific/ limited interim data (e.g. safety issue) • Members must not share interim data with anyone outside DMC • Leaks can affect • Patient Recruitment • Protocol Compliance • Outcome Assessment • Trial Support
Conclusions • Learn from history (e.g., NHLBI) • Develop DMC experience • Evolving process • “Eye on the prize” – Patient safety and protection