Download
1 / 15
160 likes | 177 Views
This study aims to link health promotion by barbers to drug therapy by pharmacists for improved hypertension control in non-Hispanic Black men. Results show significant reductions in systolic blood pressure compared to standard care practices.

E N D
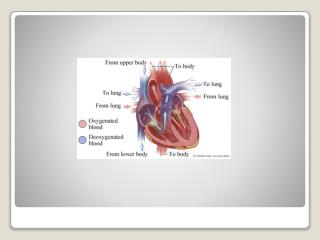
Blood-Pressure Reduction in Black Barbershops (ClinicalTrials.gov number, NCT02321618) Ronald G. Victor, M.D. Kathleen Lynch, Pharm.D. Ning Li, Ph.D. (UCLA) Ciantel A. Blyler, Pharm.D. Eric Muhammad, B.A. Joel Handler, M.D. (Kaiser) Jeffrey Brettler, M.D. (Kaiser) Mohamad Rashid, M.B.Ch.B. Brent Hsu, B.S. Davontae Foxx-Drew, B.A. Norma Moy, B.A. Anthony E. Reid, M.D. Robert Elashoff, Ph.D. (UCLA)
Background Non-Hispanic black men • Highest HTN-related death rate in the U.S. • Less physician interaction with lower HTN treatment & control rates than black women, thus necessitating community outreach Health outreach to barbershops • Well-established but …can it improve HTN control? • Prior RCT: marginally lower BP when barbers checked BP and referred patrons with high readings to primary care than when they distributed HTN pamphlets (design issues, clinicians rarely intensified drug therapy)* * Victor RG et al,. Arch Intern Med, 2011; Rader F et al. , Am J Cardiol, 2013.
Aim-to develop an effective intervention which links health promotion by barbers to drug therapy by pharmacists, and evaluate efficacy in a cluster RCT. Primary • Pharmacists’ actions have improved HTN control in > 40 RCTs in • traditional healthcare settings that included few black men • (Santschi V et al., JAHA 2014; Cheema E et al., Br J ClinPharmacol 2014) Randomized black male patrons with uncontrolled HTN by barbershop • Control Group • Barbers promoted: • follow up w/ PCPs • lifestyle modification • Intervention Group • Barbers promoted follow up w/ specialty-trained pharmacists. • Pharmacists met patrons monthly at the barbershops: • Checked BP • Prescribed medications (collaborative practice) • Monitored electrolytes • Sent progress notes to PCPs Primary Outcome: ⍙ systolic BP at 6 months
Intervention Group Medication Protocol Goal: in-barbershop BP < 130/80 mmHg = new 2017 ACC/AHA/ASH guidelines Plasma electrolytes at the point of care Step 1. CCB plus ARB or ACEI • amlodineplusirbesartan Step 2. add thiazide-type diuretic • indapamide Step 3. add aldosterone antagonist • spironolactone
Screening, Enrollment, & Data Accuracy (independent survey research company- Westat) • In-person structured laptop interviews • Automated in-barbershop BP - 5 BPs, average last 3 - automated transmission Inclusion Criteria Protocol • Non-Hispanic black men • Ages 35-79 yr. • Regular patrons (≥ 1 haircut in 6 weeks x ≥ 6 months) • SBP ≥ 140 x 2 days
319 Patrons of 52 Barbershops randomized 139 Patrons w/ uncontrolled HTN in 28 barbershops randomized to Intervention Group 180 Patrons w/ uncontrolled HTN in 24 barbershops randomized to Control Group 7 lost to follow-up 1 Deceased 6 Withdrew 9 lost to follow-up 1 Deceased 8 Withdrew 95% cohort retention 132 Participants with complete 6-month data 171 Participants with complete 6-month data
Baseline Characteristics: Participants (cont.) *By self-report, ** P=0.04
Primary Outcome: Systolic BP *Mixed linear effects model, with random intercepts for clusters, and adjusted for baseline BP, routine doctor, and high cholesterol. Drop outs were considered to be occur at random.
Secondary Outcome Comparison to Prior Studies • Net BP reduction of -21.6 /-14.9 mm Hg: • 10-15X larger than in our prior barbershop trial (-2.5/-0.9 mm Hg) • 3X larger than the average SBP effect in pharmacist intervention trials (-7 mmHg)
BP Drugs at 6 Months • Intervention vs. control group • more long-acting ARBs (or ACEIs) & CCB (amlodipine) • more indapamide (than HCTZ) • more spironolactone • less standard beta-blockers
Safety Outcomes after 6 Months • Intervention was safe & well tolerated with no SAEs • 3 cases of reversible acute kidney injury in the intervention group, all related to indapamide.
Conclusions • Medication management delivered in barbershops by specialty-trained pharmacists, as compared with standard management by primary care practices, resulted in much larger BP reductions in patrons of those shops who had hypertension. • Because hypertensive black men often have many CVD risk factors, marked reductions in BP—if sustained using our approach and then initiated widely—might reduce high HTN-related disability & death among black men in the United States.
Acknowledgements • Posthumous Dedication - Anthony Reid, M.D. • Barbers, barbershop owners, and patrons • Funding- NHLBI (R01 HL117983) NCATS (UCLA CTSI), California Endowment, Lincy Foundation, Harriet & Steven Nichols Foundation, Burns & Allen Chair, Community Relations & Development at Cedars-Sinai • DSMB - Barry Carter, Pharm.D. (Chair) Keith Ferdinand, M.D.; Bruce Turnbull, Ph.D. • NIH official- Paula T. Einhorn, M.D.