Download
1 / 10
100 likes | 214 Views
PRK. FDA approval:1995. LASIK. FDA approval:1999. Evolution of surface treatments for the correction of ametropias. Postoperative pain Late visual recovery Risk of Haze. Epithelial injury. Intrastromal incision In a deep plane in the stroma. Risk of corneal ectasia Unpredictable

E N D
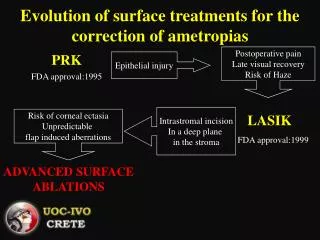
PRK FDA approval:1995 LASIK FDA approval:1999 Evolution of surface treatments for the correction of ametropias Postoperative pain Late visual recovery Risk of Haze Epithelial injury Intrastromal incision In a deep plane in the stroma Risk of corneal ectasia Unpredictable flap induced aberrations ADVANCED SURFACE ABLATIONS
Advanced Surface Ablations The term “advanced surface ablations”: • was coined as a way to explain the evolution in surface ablation techniques from the earlier PRK days • covers several techniques such as: • PRK with the intraoperative use of mitomycin-C (MMC) (PRK-MMC) • epipolis LASIK (Epi-LASIK) • laser epithelial keratomileusis (LASEK)
Advanced Surface Ablations Advanced surface ablation techniques offer several advantages over conventional PRK such as: • increased quality of vision • reduced postoperative pain • minimized corneal haze
Advanced Surface Ablations Reasons for selecting a surface treatment: • Thin corneas for attempted correction (residual bed thickness < 300μm) • Preoperative Dry Eye • Epithelial basement membrane dystrophies • Flat or steep corneas • No risk of flap-related complications • No risk of flap-induced aberrations
Epithelial Removal The epithelium can be removed with several ways: • Mechanical removal of the epithelium with a blade or newly a rotating brush • Epithelial removal with the use of alcohol (LASEK) • Epi-LASIK • Epithelial removal with the laser (transepithelial)
Evolution ofAdvanced Surface Ablations (I) • Introduction of MMC for the control of corneal haze: • Therapeutic use globally accepted (selected complicated cases) • Intraoperative prophylactic use after PRK (PRK-MMC)
Evolution ofAdvanced Surface Ablations (II) • Introduction to the retained epithelial flaps (LASEK, Epi-LASIK): • Allow for decreased incidence of haze • Offer with better tolerance of patients • Mechanical epithelial separation provides with the benefit of avoiding alcohol toxicity
PRK-MMC • 0.02% for up to 1.5 min depending on the attempted correction (delay in epithelial healing at 2 min) • Reduction of myofibroblast activity / haze (compared to corticosteroids) • Faster visual recovery and confocal microscopic normalization • Safety up to about 10 yrs max experience
LASEK • A dilute solution (20%) is used on the eye in a holding cup (8.5mm diameter) for approximately 30 seconds in order to loosen the epithelium and creates a complete epithelial flap • After the loosened epithelium is slid to the side and the stromal surface is treated with the laser • The epithelium is replaced or can be directly removed
Epi-LASIK • Surface ablation (epi-polis superficial) • Epithelium is separated as a sheet and replaced on the ablated stroma • Special device (Epikeratome) - automated procedure • No use of alcohol • Dealing with drawbacks of PRK (postoperative pain/ discomfort, late visual recovery, haze) and avoiding risks of LASIK • Suitable for thin corneas