Download
1 / 222
2.22k likes | 2.49k Views
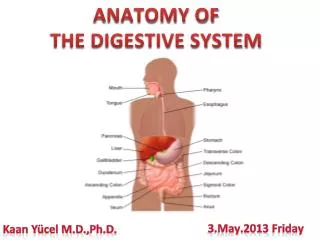
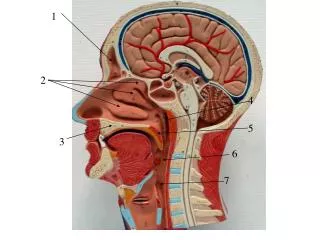
ORAL HEALTH AND DENTISTRY . The anatomy of the oral cavity and salivary glands. Borders: roof = palate (hard, soft) floor = tongue, mucosa, geniohyoid and mylohyoid m Lat/ant Outer fleshy wall = cheeks, gums Inner bony wall = teeth and inner aspect of gums

E N D
ORAL HEALTH AND DENTISTRY The anatomy of the oral cavity and salivary glands. • Borders: • roof = palate (hard, soft) • floor = tongue, mucosa, geniohyoid and mylohyoid m • Lat/ant • Outer fleshy wall = cheeks, gums • Inner bony wall = teeth and inner aspect of gums • communicates posteriorly with oropharynx • Divided into 2 areas: the oral vestibule, anterior to the teeth and buccal side of gingiva (gums) & oral cavity proper, which is the space behind the teeth and gums
Oral Vestibule = Cheeks, Lips, Gingivae Lips Lips contain theorbicularisoris m, and sup/inf labial m, a/v/n. Covered externally by skin externally, and mucosa internally. Epithelium of skin transitions from normal skin –> red vermillion portion –> to inner mucosal layer. The border line b/w skin and red portion = transition zone.
Structures to identify in relation to the lips: upper lip = b/w nose & opening of oral cavity nasolabial grooves = seperate lips from cheeks, 1 cm lat to angle of mouth philtrum = a shallow depression below the nose, bordered by 2 lateral crests – not everyone has one lower lip = b/w opening of oral cavity and labiomental groove, separating lower lip from chin. labial frenula = a mucosal membrane fold that attaches the lips to the ant surface of the vestibular gingiva (gums facing the oral vestibule) — NOTE diff from lingual frenula, that attaches the tongue to the floor of the mouth
Blood supply = sup/inf labial a (facial a) upper lip = br of facial/ infraorbital = sup labial br lower lip = br of facial/mental a = inf labial br Innervation upper lip = sup labial br of V2 lower lip = inf labial br of mental n from V3 (mental n comes from infalveloar n) Lymph Drainage = submandibular/submental lymph nodes
Cheeks over lie thezygomatic processcontain the buccinator m - that holds cheeks taught when exhaling forcefullycontains the buccal fat pad (of Bichat)Blood Supply = buccalbr of maxillary a (terminal br of ext carotid), n = buccalbr of mandibular n (V3)
Gums are fibrous tissue covered with mucosahold teeth in placesupplied by many a/v/n Blood Supply upper (maxillary) lingual gingivaof incisors, canines = nasopalatinen,a/v – most ant, this makes sense because nasopalatine structures go through incisive foramen at most ant part of hard palate upper (maxillary) lingual gingiva of premolars, molars = gr. palatine n, a/v – post, makes sense b/c gr. palatine structures go through gr palatine foramen at post/lat part of hard palate lower(mandibular) labial buccalgingiva of incisors, canines, premolars =inf alveolar n/a/v lower(mandibular) labial buccalgingiva of molars = buccal n lower(mandibular) lingual gingiva = lingual n/a/v
Palate Made up of hard and soft palate Hard palateis bony and makes up the ant 4/5 of the palate = palatine process of the maxilla, and horizontal plate of palatine boneborder b/w nasal and oral cavity@ midline of hard palate, running back from incisive foramen = palatine raphe – where the 2 palatine shelves fused in embryonic life 3 foramina:Incisive foramen (ant/med) = nasopalatine n/a/v In the netter, it looks like sphenopalatine a goes through there, but do not say this in a test, it will be considered incorrect. NOTE – makes the location of the fusion b/w primary/secondary palate in embryonic life Greater and Lesser Palatine foramen (post/lat) – right next to 3rd molar (wisdom tooth) = the gr/lsr palatine n/a/v go through them. Gr palatine structures run ant and supply hard palate Lsr palatine stuctures run post and supply soft palate The a comes from desc palatine a, a br of maxillary a
Soft Palate • is fibromuscular fold that makes up post 1/5 of palate • moves agains the pharyngeal wall to close oropharynx while swallowing or speaking • as mentioned earlier, supplied a/v/n by lesser palatine structures. • Laterally, is continuous with palatoglossal and palato pharyngeal folds • These folds are form the lateral border to the exit of oral cavity = Isthmus of Fauces, that leads to Oropharynx (More on that in pharynx) • b/w them is the tonsillar bed = palatine tonsils • CLINCAL NOTE – are frequently inflamed and removed, along with pharyngeal tonsils (see pharyn) aka adenoids • CLINCAL NOTE = Since lingual gingiva is connected to mucosa of soft palate, can inject anasthetic there to numb soft palate • Has numerous palatine glands, that secrete mucus • Blood Supply:Gr and Lsr palatine a (more the 2nd one), Asc palatine a (Facial a), Palantinebr of Asc Pharyngeal a • Innervation : SS = lsr palatine n, SM = CN X • Venous Drainage: hard and soft palate v drain in pterygoid venous plexus • NOTE that Hard palate has no SM innervation – no musc there.
Muscles of Palate: all innervated by CN X via pharyngeal plexus – except Tensor VeliPalatini (V3) Tensor VeliPalatini- tenses soft palate, has a large tendon that strengthens the soft palate = palatine aponeurosis LevatorVeliPalatini – elevate soft palate Palatoglossus- elevates tongus (Just uses palate as an origin site, doesn’t do anything to palate itself) Palatopharyngeus – elevates pharynx, to help close off nasopharynx from oropharynx in swallowing Uvulus – @ termination of soft palate, no real function, but helps to identify issues with CN X, b/c if this doesn’t move when saying, “Ahhh”, then poss malfunction w. CN X
Tongue • is almost purely made of muscle • the ant 2/3 is called the oral part = originates from 1st pharyngeal arch • post 1/3 = pharyngeal part, orginates from 3rd arch, behind terminal sulcus of tongue • @ midline of terminal sulcus is foramen cecum, the remnant of thyroglossal duct • root = from 4th arch • Has midline sulcus on dosal surface = location of fusion of 1 lateral swellings of ant tongue over tuberculumimpar. Function: aid in speaking, allow for movement of food toward oropharynx and within oral cavityParts:Body – most of the tongueApex – pointed ant partroot – part fixed to hyoid bone and mandible, is located behind palatoglossal fold, location of lingual tonsils.
Taste Buds: SEE HISTO The inferior surface of tongue has a very thin mucus membrane, so can see many veins, and is attached to floor of mouth via another mucus membrane fold = lingual frenulum. – Basically keeps tongue in mouth while allowing apex to move about Muscle of Tongue = all innervated by CN XII, except palatoglossus, which we already said is innervated by Pharyngeal plexus, via CN X Intrinsic m - change the shape of tongue itselfSup/Inf Longitudinal, Transverse, Vertical Extrinsic m – change position of tongue Genioglossus – protrudes and depresses tongue Hyoglossus – depresses and retracts tongue Styloglossus – retracts and elevate tongue Palatoglossus – elevates tongue
How to remember them? Gay Hats STYLe Perfectly Basic Taste sensations:Sweetness = apexSaltiness = lateral sideSourness & bitterness = posterior partUmami = used to taste the unusual tastes in cheese, meat, asparagus, & tomatoes Blood Supply: Lingual a from Ext carotid a, emerges @ lever of gr. horn of hyoid bone in carotid triangle Pathway: runs deep to hyoglossis (lateral lingual groove), and lies on middle pharyngeal constrictorm Br = dorsal lingual, suprahyoid,sublingual a, terminates as deep lingual a ( on top of genioglossus m) Lymph Drainage: Post 1/3 = deep cervical lymph nodes Medial ant 2/3 = inf deep cervical lymph nodes lat ant 2/3 = submandibularl.n apex = submentall.n Innervation of Tongue: Ant 2/3: SS = CN V3 via Lingual n, VS = CN VII via Chorda Tympani Post 1/3: SS/VS = CN IX Root: SS = CN X, no taste buds here, so no VS
Salivary Glands: Parotid Location: Retromandibular Space = Parotid BedBorders: ant = Masseter m, Ramus of mandible post = SCM, post digastric m sup = zygomatic arch inf = fascia b/w SCM and mandible Lat = open General Info:covered by dense fibrous capsule from investing fascia of necksecretes serous salivalargest of the glands secretion of gland
Duct Pathway:From widest part of gland –> across masseter and deep to it –> lat/ant to Buccal fat pad –> peircesBuccinator m, and opens @ 2nd maxillary (upper) molar Structures Passing through It:Ext Carotid a - giving 2 terminal branches = Maxillary a, Superficial temporal aSuperficial Temporal v & Maxillary v combine to give Retromandibular vFacial npeirces it and gives 5 terminal branches – DOES NOT innervate the glandAuriculo temporal n – carries PNS post synaptic fibers with it to increase secretion of gland
Blood supply:from branches of external carotid and superficial temporal a = Transverse facial aVeins follow a and drain into Retromandibular v Lymph Drainage:superficial and deep cervical lymph nodesInnervation: Tympanic n arises from CN IX and emerges from jugular foramen n enters the middle ear via the tympanic canaliculus in petrous part of temporal bone tympanic n forms the tympanic plexus — and lesser petrosal n emerges from this plexus lesser petrosal leaves skull via foramen ovale PNS fibers from it synapse in otic ganglion post ggl fibers from ggl RUN W/ auriculotemporal n (from V3) to supply parotid gland *Parotid and Submandibular gland separated by stylomandibularligb/w styloid process & angle of mandible
Submandibular GlandLocated: below mylohyoid & mandible General Info:Has Superficial and Deep part (deep part located b/w mylohyoid and styloglossus)secretes a mix of serous and mucus saliva Duct Pathway:ducts runs thru lat space of tongue w/ Hypoglossal n and lingual n = lateral lingual groove —> then eventually goes to and open lat to frenulum, b/w mylohyoid and styloglosseslingual n loops under duct in the lateral lingual groove Blood Supply:sunmental a (Facial a), V run with a. Lymph Drainage: deep cervical l.n. –> jugulo-omohyoid nodes Innervation:Pre ggl PNS fibers from CN VII by chordatympani –> submandibularggl –> post ggl fibers run w/ lingual nSNS post ggl fibers come from sup cervical ggl
Sublingual GlandsLocation: b/w mandible and genioglossus m General info:smallest of the 3 glandssecretes both mucus and serous, but more mucus Duct Pathway: duct opens @ floor of oral cavity w/ submandibular duct, just below mucus membrane of tongue, lat to frenulum Blood Supply : Submental and sublingual a (from facial and lingual a) Innervation:Pre ggl PNS fibers from CN VII by chordatympani –> submandibularggl –> post ggl fibers run w/ lingual n SNS post ggl fibers come from sup cervical ggl
Evaluation and examination of oral cavity Physical Examination of the Oral Cavity • Lips • Inspect landmarks – vermilion zone, commissures, nasolabial fold • Inspect color • Inspect surface for ulcerations, blisters, growths, thickness changes • Observe patient with mouth closed and patient smiling to look for cranial nerve VII lesions • Palpate with gloved hands for surface irregularities not visible to the eye, submucosal nodules, and areas of tenderness • Labial mucosa – reflect lips with gloved hands • Inspect color and surface for nodules, ulcerations, thickenings • Palpate upper and lower surfaces with two fingers from commissure to commissure to detect submucosal changes
Buccal mucosa – have patient open mouth wide in order to inspect and have good lighting. • Inspect color and surface for nodules, ulcerations, thickenings • Identify normal landmarks: pterygomandibularraphe and parotid papilla. Identify parotid papilla on mucosal surface near upper molars. Palpate the parotid gland and observe for expression of fluid from Stensen’s duct • Palpate surface with two fingers to identify submucosal lesions • Gingiva and alveolar mucosa
Gingiva and alveolar mucosa • inspect color of gingival and alveolar mucosa. • Inspect texture of gingival and alveolar mucosa – look for atrophy, recession, hypertrophy or enlargement. Look for ulcerations. • Palpate any areas of enlargement to determine if enlargement is due to edema, or an underlying bony or fibrous process
Palate • identify hard and soft palate landmarks – fovea palatinae, palatine raphe, alveolar tuberosity, hamular notch, pillars of the fauces, uvula. Inspect for any developmental abnormalities of these landmarks • Inspect color of hard and soft palate and inspect for ulcerations, thickenings, exudates. petechiae • Palpate posterior hard palate and soft palate for subcutaneous nodules
Tongue – inspect in normal resting position and in a protruded position • Identify landmarks: terminal sulcus, median sulcus, foramen cecum, lingual frenulum • Be familiar with normal appearance of filiform, fungiform and circumvallate papillae • Inspect color and texture of dorsal, ventral and lateral surfaces. Look for plaques, ulcerations, thickenings, changes in papillae • Palpate dorsal and ventral aspects of the tongue • Evaluate movement of tongue
Floor of the Mouth – have patient open mouth touch tip of tongue to roof of mouth to inspect. Carefully retract tongue to inspect distal aspects of floor. • inspect normal landmarks – lingual frenulum, sublingual folds, caruncles • inspect for color and texture changes • palpate entire sublingual and submandibularfossa areas by bimanual palpation to detect nodules, differences in consistency of sublingual glands and tissues • Teeth • Inspect for number and position of teeth – understand how the number of teeth change from childhood to adulthood, look for changes in teeth structure or number that indicate congenital/genetic syndromes • Inspect color of teeth and look for surface changes indicative of early dental decay
Orlal examination Scope of responsibility Diseases of the head & neck Diseases of the supporting hard & soft tissues Diseases of the lips, tongue, salivary glands, oral mucosa Diseases of the oral tissues which are a component of systemic disease
Many diseases (systemic or local) have signs that appear on the face, head & neck or intra-orally Making a complete examination can help you create a differential diagnosis in cases of abnormalities and make treatment recommendations based on accurate assessment of the signs & symptoms of disease
Equipment • Assure that you have all the supplies necessary to complete an oral examination • Mirror • Tissue retractor (tongue blade) • Dry gauze • You must dry some of the tissues in order to observe the nuances of any color changes
Extra-oral examination • Observe: color of skin • Examination area of head & neck • Determine: gross functioning of cranial nerves • Normal vs. abnormal • Paralysis • Stroke, trauma, Bell’s Palsy
TMJ • Palpate upon opening • What is the maximum intermaxillary space? • Is the opening symmetrical? • Is there popping, clicking, grinding? • What do these sounds tell you about the anatomy of the joint? • When do sounds occur? • Use your stethoscope to listen to sounds
Lymph node palpation • Refer to handout
Thyroid Gland Palpation • Place hands over the trachea • Have the patient swallow • The thyroid gland moves upward
Exam: Lips Observe the color & its consistency-intra-orally and externally Is the vermillion border distinct? Bi-digitally palpate the tissue around the lips. Check for nodules, bullae, abnormalities, mucocele, fibroma
Evert the lip and examine the tissue Observe frenum attachment/tissue tension Clear mucous filled pockets may be seen on the inner side of the lip (mucocele). This is a frequent, non-pathologic entity which represents a blocked minor salivary gland
Exam: Lips-palpation • Color, consistency • Area for blocked minor salivary glands • Lesions, ulcers
Frenum: • Attachment • Level of attached gingiva
Examination: Buccal Mucosa • Observe color, character of the mucosa • Normal variations in color among ethnic groups • Amalgam tattoo • Palpate tissue • Observe Stenson’s duct opening for inflammation or signs of blockage • Visualize muscle attachments, hamular notch, pterygomandibular folds
Linea alba • Stenson’s duct
Lesions – white, red • Lichen Planus, Leukedema
Gingiva Note color, tone, texture, architecture & mucogingival relationships
How would you describe the gingiva? • Marginal vs. generalized? • Erythematous vs. fibrous • Drug reactions: Anti-epileptic, calcium channel blockers, immunosuppressant
Exam: Hard palate • Minor salivary glands, attached gingiva • Note presence of tori: tx plan any pre-prosthetic surgery
Exam: Soft palate • How does soft palate raise upon “aah”? • Vibrating line, tonsilar pillars, tonsils, oropharynx
Exam: Oropharanyx • Color, consistency of tissue • Look to the back, beyond the soft palate • Note occasional small globlets of transparent or pink opaque tissue which are normal and may include lymphoid tissue
Exam: Tonsils • Tucked in at base of anterior & posterior tonsilar pillars • Globular tissue that has “punched out” appearing areas • Regresses after adulthood • May see white “orzo rice like” or “torpedo” shaped white concretions within the tissue