Download
1 / 1
10 likes | 136 Views
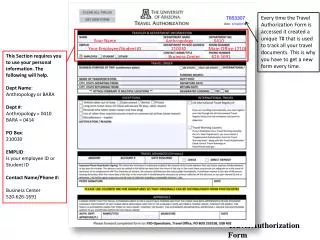
This Medical Emergency Authorization Form grants permission for VBS Directors or staff representatives of the First Apostolic Church to seek medical treatment for your child during the Vacation Bible School program from June 23-27, 2008. The form collects essential information including the child's name, age, grade, medical history, allergies, current medications, and insurance details. A signature from a parent or guardian is required, ensuring that appropriate consent is provided for any necessary medical interventions.

E N D
Medical Emergency Authorization Form I, the undersigned, hereby authorize the VBS Directors or VBS staff representative of the First Apostolic Church to consent to and authorize the administration and performance of all treatments that may be considered advisable or necessary in the judgment of an attending physician, in the event that my child should be admitted to any hospital, or be in need of any medical treatment. This authorization shall continue for such time as they are participating in the Vacation Bible School Program, June 23-27, 2008. Childs Name: ______________________________ Age:____________________ Grade entering this fall:________________________________________________ Address:__________________________________________________________ __ City, State, Zip:_______________________________________________________ Home phone: ______________________________ Cell Phone:______________ Insurance carrier:___________________________ Security Password: _______________________________ (To be used when picking up your child each evening) Health History Does your child have any conditions that would prevent him or her from participating in any of the VBS activities? Yes No __ (If yes, please explain) Allergies to food, medication, environment? Yes______ No __ (If yes, please explain) Current medications: _____________________________________________ Please use the space below or the back of this form to indicate anything else that the VBS team should know to help avoid or assist in any medical situation that might arise. Parent/Guardian signature:_________________________________________ Date:_________________