Download
1 / 1
10 likes | 123 Views
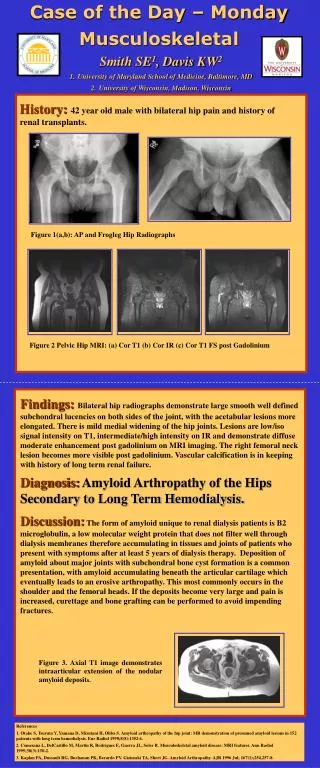
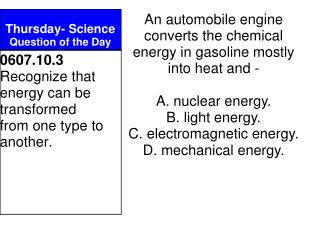
Case of the Day – Thursday MUSCULOSKELETAL. Andrew J. Ziegert, MD 1 , Kirkland W. Davis 1 , MD, Stacy E. Smith, MD 2 1 University of Wisconsin Medical School, Madison, Wisconsin 2 University of Maryland Medical System, Baltimore, Maryland. History: 32 year old female with knee pain. (b).

E N D
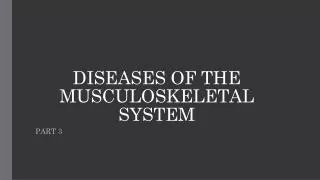
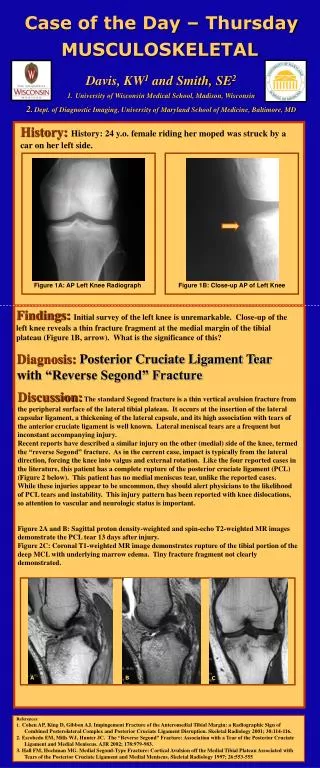
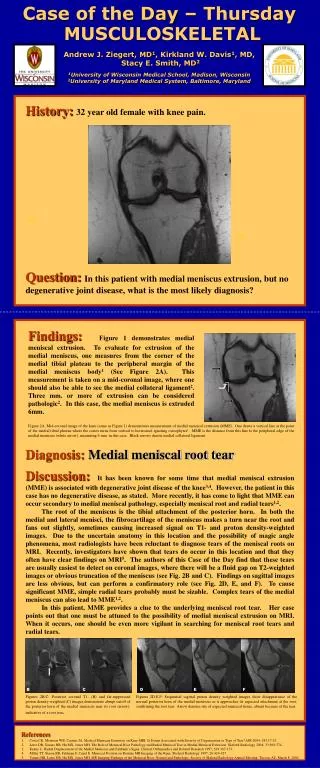
Case of the Day – Thursday MUSCULOSKELETAL Andrew J. Ziegert, MD1, Kirkland W. Davis1, MD, Stacy E. Smith, MD2 1University of Wisconsin Medical School, Madison, Wisconsin 2University of Maryland Medical System, Baltimore, Maryland History:32 year old female with knee pain. (b) (a) (c) Question:In this patient with medial meniscus extrusion, but no degenerative joint disease, what is the most likely diagnosis? Findings:Figure 1 demonstrates medial meniscal extrusion. To evaluate for extrusion of the medial meniscus, one measures from the corner of the medial tibial plateau to the peripheral margin of the medial meniscus body1 (See Figure 2A). This measurement is taken on a mid-coronal image, where one should also be able to see the medial collateral ligament2. Three mm. or more of extrusion can be considered pathologic2. In this case, the medial meniscus is extruded 6mm. Figure 2A: Mid-coronal image of the knee (same as Figure 1) demonstrates measurement of medial meniscal extrusion (MME). One draws a vertical line at the point of the medial tibial plateau where the cortex turns from vertical to horizontal, ignoring osteophytes1. MME is the distance from this line to the peripheral edge of the medial meniscus (white arrow), measuring 6 mm. in this case. Black arrows denote medial collateral ligament. Diagnosis:Medial meniscal root tear Discussion:It has been known for some time that medial meniscal extrusion (MME) is associated with degenerative joint disease of the knee3,4. However, the patient in this case has no degenerative disease, as stated. More recently, it has come to light that MME can occur secondary to medial meniscal pathology, especially meniscal root and radial tears1,2. The root of the meniscus is the tibial attachment of the posterior horn. In both the medial and lateral menisci, the fibrocartilage of the meniscus makes a turn near the root and fans out slightly, sometimes causing increased signal on T1- and proton density-weighted images. Due to the uncertain anatomy in this location and the possibility of magic angle phenomena, most radiologists have been reluctant to diagnose tears of the meniscal roots on MRI. Recently, investigators have shown that tears do occur in this location and that they often have clear findings on MRI5. The authors of this Case of the Day find that these tears are usually easiest to detect on coronal images, where there will be a fluid gap on T2-weighted images or obvious truncation of the meniscus (see Fig. 2B and C). Findings on sagittal images are less obvious, but can perform a confirmatory role (see Fig. 2D, E, and F). To cause significant MME, simple radial tears probably must be sizable. Complex tears of the medial meniscus can also lead to MME1,2. In this patient, MME provides a clue to the underlying meniscal root tear. Her case points out that one must be attuned to the possibility of medial meniscal extrusion on MRI. When it occurs, one should be even more vigilant in searching for meniscal root tears and radial tears. B C D E F Figures 2B,C: Posterior coronal T1- (B) and fat-suppressed proton density-weighted (C) images demonstrate abrupt cutoff of the posterior horn of the medial meniscus near its root (arrow), indicative of a root tear. Figures 2D,E,F: Sequential sagittal proton density weighted images show disappearance of the normal posterior horn of the medial meniscus as it approaches its expected attachment at the root, confirming the root tear. Arrow denotes site of expected meniscal tissue, absent because of the tear. References Costa CR, Morrison WB, Carrino JA. Medical Meniscus Extrusion on Knee MRI: Is Extent Associated with Severity of Degeneration or Type of Tear? AJR 2004; 183:17-23. Lerer DB, Umans HR, Hu MX, Jones MH. The Role of Meniscal Root Pathology and Radial Meniscal Tear in Medial Meniscal Extrusion. Skeletal Radiology 2004; 33:569-574. Kenny C. Radial Displacement of the Medial Meniscus and Fairbank’s Signs. Clinical Orthopaedics and Related Research 1997; 339:167-173. Miller TT, Staron RB, Feldman F, Cepel E. Meniscal Position on Routine MR Imaging of the Knee. Skeletal Radiology 1997; 26:424-427. Umans HR, Lerer DB, Hu MX, Jones MH. MR Imaging Findings of the Meniscal Root: Normal and Pathologic. Society of Skeletal Radiology Annual Meeting; Tucson, AZ, March 8, 2004.