Discussion
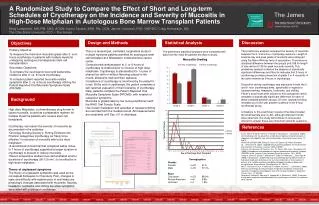
Background. Methods. Table 1: Baseline Demographic Characteristics of Study Cohort. Table 2: Factors Associated with Off-Label CRT Implantation (Hierarchical Logistic Regression). Figure 2: Time Trend of Off-Label CRT-D Implantation. Conclusions. Results. Figure 1: Investigational Design.

Discussion
E N D
Presentation Transcript
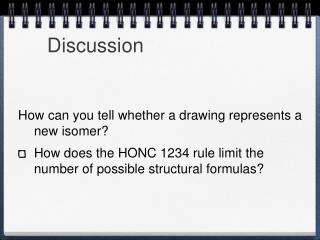
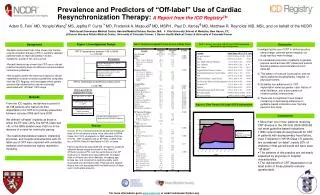
Background Methods Table 1: Baseline Demographic Characteristics of Study Cohort Table 2: Factors Associated with Off-Label CRT Implantation (Hierarchical Logistic Regression) Figure 2: Time Trend of Off-Label CRT-D Implantation Conclusions Results Figure 1: Investigational Design Discussion Prevalence and Predictors of “Off-label” Use of Cardiac Resynchronization Therapy:A Report from the ICD RegistryTM Adam S. Fein* MD, Yongfei Wang¥ MS, Jeptha P. Curtis ¥ MD, Frederick A. Masoudi†MD, MSPH , Paul D. Varosy╬ MD, Matthew R. Reynolds* MD, MSc, and on behalf of the NCDR *Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA; ¥ Yale University School of Medicine, New Haven, CT; ╬ Denver Veterans Affairs Medical Center, University of Colorado Denver; † Denver Health Medical Center & University of Colorado Denver Investigating the use of CRT in clinical practice using a large, national patient registry, our study had four main findings: A substantial proportion of patients in general practice received new CRT placement outside clinical guideline recommendations from 2006-08. This pattern of overuse is pervasive, and not easily explained by geographic, hospital, or physician factors. Guideline non-adherence for CRT implantation varies by gender, race, history of atrial fibrillation, and a prior pattern of invasive cardiac interventions. There was no significant trend toward increasing or decreasing adherence to guideline-based indications over the time period of this study. • Multiple randomized trials have shown that cardiac resynchronization therapy (CRT) in carefully selected patients leads to improved cardiac function, symptoms, quality of life, and survival. • Recent literature has shown that CRT use in clinical practice frequently does not adhere to evidence-based consensus guidelines. • We sought to define the extent and nature of device implantation outside consensus guidelines using data from the ICD Registry, and investigate which patient and provider related factors are most strongly associated with “off-label” CRT usage. CRT-D Implantations between 1/06 to 06/08 n = 105,543 • Exclusions Previous pacemaker (n= 13,622) or ICD (n= 23,479) ICD for Secondary Prevention (n=14,431) or history of cardiac arrest (n =954), sustained VT (n=1,035), or syncope (n=5,420) CRT-D Implantations Identified as Study Cohort (n=46,198) OFF-Label CRT-D Implantation Group EF was >35% (n = 601) NYHA Class was < III (n=6,081) From the ICD registry, we defined a cohort of 46,198 patients who had a first-time implantation of a CRT-D for primary prevention between January 2006 and June 2008. We defined “off-label” implants as those in which the EF was >35%, the NYHA Class was <III, or the QRS duration was ≤120 ms in the absence of a need for ventricular pacing. The relationships between patient, implanting physician, and hospital characteristics with off-label use of CRT were explored with univariate statistics and hierarchical logistic regression modeling. QRS duration ≤120 ms without a need for ventricular pacing (n=7,619) 33,408 CRT-D Implantations in Adherence with ACC/AHA Guidelines • More than one in four patients receiving CRT devices in the US from 2006-2008 did not meet guideline based indications. • With recent trials showing benefit for CRT in patients with asymptomatic heart failure, even if implants in NYHA Class I /II patients are considered “on-label”, nearly 20% of implants in that period would still have been “off-label”. • The patterns of this practice are not easily explained by physician or hospital characteristics. • The risk-benefit of CRT implantation in at least some of these patients remains questionable Overall, 27.7% of devices were placed without meeting all three of the consensus criteria, most often due to NYHA Class <III (13.2% of implants) or QRS duration ≤120 ms (16.7%). CRT recipients had an EF>35%, a QRS ≤100 ms, or NYHA Class ≤I heart failure in 8.0% of cases. Factors significantly associated with off-label vs. guideline adherent device usage are shown in the Table 2. AF/flutter, previous PCI, and the performance of an EP study prior to implant were associated with increased odds of off-label use, while diabetes, increasing age, female sex, and nonischemic cardiomyopathy were associated with decreased odds. Physician and hospital factors were not associated with the likelihood of off-label use in multivariate analysis. For more information go to www.ncdr.com or email ncdrresearch@acc.org