Discussion
Eaten from the Inside: A Rare Case of Disseminated Strongyloides Infection Arbi Ayvazian D.O., Michael Neeki D.O., Pamela Lux D.O. Arrowhead Regional Medical Center, Department of Emergency Medicine. Hospital Course.

Discussion
E N D
Presentation Transcript
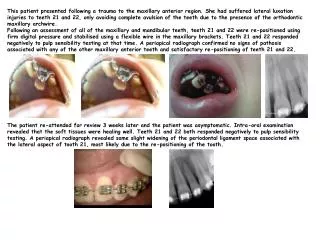
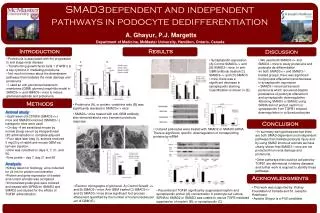
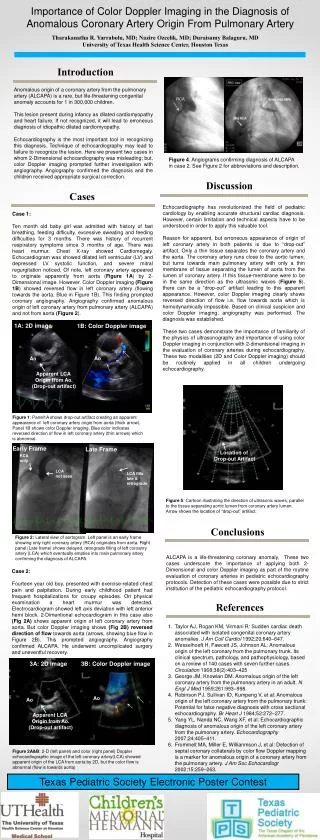
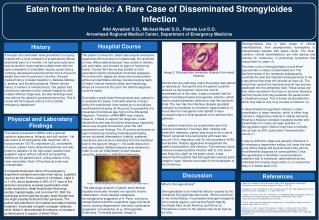
Eaten from the Inside: A Rare Case of Disseminated Strongyloides InfectionArbi Ayvazian D.O., Michael Neeki D.O., Pamela Lux D.O.Arrowhead Regional Medical Center, Department of Emergency Medicine Hospital Course . Strongyloidiasis has a wide range of clinical manifestations, from asymptomatic eosinophilia to disseminated disease with septic shock. The most-common clinical manifestations are mild waxing and waning GI, cutaneous, or pulmonary symptoms that may persist for years (1). History A 59-year-old Cambodian male presented to a county hospital with a chief complaint of progressively diffuse abdominal pain for 2 months. He had previously been seen at another local hospital multiple times with the same complaints of intractable nausea, green bilious vomiting, decreased bowel movement and a 20-pound weight loss over the previous 2 months. His past medical history included hepatitis C, diabetes Mellitus 2, anemia, and thrombocytopenia. Patient denied history of melena or hematochezia. The patient had recent prior admission at an outside hospital for with multiple different diagnoses, but was discharge each time without the patient’s symptoms improving. This of course led his frequent returns to the outside emergency department. The patient continued to deteriorate despite exhaustive supportive efforts during his hospital stay. He remained to have diffuse abdominal pain, was unable to tolerate any oral intake, and showed no signs of functioning bowel. During this time he was started on total parenteral nutrition and patient controlled analgesia. He continued to display an obstructive-bowel pattern without an identifiable etiology. General surgery team, GI team, Internal medicine team, and Hepatology where all involved at this point. No definite diagnosis could be made. Eventually a small bowel through study was ordered to re-evaluate the bowel. It showed retained contrast within the small-bowel (from weeks prior) and diffuse small-bowel thickening. At this point, the possibility of a mesenteric thrombosis was high on the differential diagnosis. Therefore a MRA/MRV was ordered, however, it failed to support the diagnosis. It was decided the next step should be endoscopy, especially before any surgical intervention given the odd presentation and findings. The GI service performed an upper endoscopy showing moderate gastropathy, severe duodenal inflammation, friability, scattered ulcerations and erosions extending from the duodenal bulb to the jejunum (Image 1). No outlet obstruction was appreciated. Multiple biopsies were obtained in order to rule out inflammatory bowel disease, vasculitis, ischemia or infiltrative lymphoma. The main route of strongyloidiasis occurs when exposed skin contacts contaminated soil. The filariform larvae of the nematode subsequently penetrate the skin and migrate hematogenously to the lungs where they enter the alveolar air sacs (4). The larvae then ascend the tracheobronchial tree and are swallowed into the alimentary tract. These larvae are then either secreted in the feces or become infectious filariform larvae that may penetrate the perianal skin or intestinal mucosa. This is known as autoinfection, which may lead to very long courses of infection (4). In disseminated strongyloides infection a major complication is hyper-infection, which is either drug induced or triggered by defects in cellular immunity. Allowing a massive increase in parasite burden and dissemination to nearly all organ systems (1). Strongyloides hyper infection may have a mortality rate as high as 90%, particularly if dissemination occurs (1). It may be difficult to diagnosis parasitic infections in an emergency department setting, but never the less good history taking and physical exam may narrow the differential diagnosis for some patients. Once Strongyloidiasis is identified, current preferred treatment with is ivermectin, administered as two individual 200 mcg/kg doses either on 2 consecutive days or 2 weeks apart (2,5). Image 2: Strongyloides nematode biopsied from small intestine. Shortly after the pathology report the patient was started on albendzole. During this time the patient condition showed no improvement. Given the clinical manifestations of this case, it was concluded that the patient had disseminated strongyloides infection, which lead to partial alimentary obstruction and this cachectic state. The next day the infectious disease specialist changed his treatment to ivermectin. Approximately 12 hours later the nasogastric tube started to have increased output of what appeared to be sediment like particles. The patient remained to be symptomatic given his extensive treatment. Few days after initiating anti-helminthic treatment, patient was found to be in shock. Patient remained to be tachycardic with heart rate around 120’s, respiratory rate 25, blood pressure 90/68, and afebrile. Despite aggressive management the patient succumbed to this infection. Post mortem, blood cultures revealed positive infection with E. Coli, which was likely the culprit for his septic shock. It was determined the patient had Strongyloides induced gram-negative hyper infection secondary to the breakdown of his GI barriers. Physical and Laboratory Findings The patient presented to ARMC with a general cachectic appearance, lethargic and soft-spoken. He was found to be tachycardic with heart rate 130’s, blood pressure 105/78, respirations 22, and afebrile. On exam, patient had a distended abdomen and was tender to palpation to the right upper quadrant and epigastric region without rebound and guarding. Additional, the patient had 2+ pitting edema in the lower extremities. Rest of the physical exam was unremarkable. A complete blood work done in the emergency department revealed some abnormal values, a platelet count of 40,000 TH/ml, sodium of 123 Meq/L, HgA1C of 11.4%, and a bandemia of 28%. A CT scan of the abdomen and pelvis revealed questionable small bowel obstruction, distal small bowel thickening, ascites, hepatomegaly, and a narrow IVC. Both the radiologist and the general surgery team thought that this might possibly be Budd Chiari syndrome. The patient was admitted to the hospital and stated medical treatment. Eventually a hepatic venogram obtained, which failed to demonstrated thrombosis or increased portal pressure in support of Budd Chiari. Discussion References Image 1: Proximal duodenum with multiple ulcerations and friable regions. The pathologic analysis of gastric and intestinal biopsies eventually revealed non-specific chronic inflammation, focal intestinal metaplasia, microorganisms suggestive of H. Pylori, and many intraepithelial helminthic organisms (eggs and larval forms) showing degeneration and micro calcification suggestive of nematodes (ie.g., Strongyloides, Enterobius, Trichinella species) (image 2). What is Strongyloidiasis? Strongyloidiasis is an intestinal infection caused by the nematode Strongyloides stercoralis. While uncommon in the United States, it is prevalent amongst immigrants from tropical regions, such as the Pacific Islands, Southeast Asia, South America, and Africa (3). Prevalence in some of the regions may be as high as 40-60%. 1. Adam, M., O. Morgan, C. Persaud, and W. N. Gibbs. 1973. Hyperinfection syndrome with Strongyloides stercoralis in malignant lymphoma. Br. Med. J. 1:264-266. 2. Archibald, L. K., N. J. Beeching, G. V. Gill, J. W. Bailey, and D. R. Bell. 1993. Albendazole is effective treatment for chronic strongyloidiasis. Q. J. Med. 86:191-195 3. Gyorkos, T.W., Genta, R.M., Viens, P., Maclean, J.D. Seroepidemiology of Strongyloides infection in the Southeast Asian refugee population in Canada. AM J Epidemiology. 1990; 132:257 http://www.ncbi.nlm.nih.gov/pubmed?term=2196791 4. Link, K., and R. Orenstein. 1999. Bacterial complications of strongyloidiasis: Streptococcus bovis meningitis. South. Med. J. 92:728-731. 5. Marti, H., H. J. Haji, L. Savioli, H. M. Chwaya, A. F. Mgeni, J. S. Ameir, and C. Hatz. 1996. A comparative trial of a single-dose ivermectin versus three days of albendazole for treatment of Strongyloides stercoralis and other soil-transmitted helminth infections in children. Am. J. Trop. Med. Hyg. 55:477-481.